McCamy Taylor
McCamy Taylor's JournalF the Supreme Court of the United States!
(In)Justice Roberts and associates forced urban voters in Wisconsin to put their lives at risk in order to exercise their Constitutional right to vote. And now the Supreme Court says it will do teleconference hearings due to COVID concerns.
I am beyond furious. Apparently the only lives that matter in this country are those on the Supreme Court.

Penny Wise and Pound Foolish: COVID PPE/Protection in Public Health Sector
Right now the nation's big public health systems have a bit of a COVID problem. They would love to keep doctors/nurses/techs/patients safe. However, being part of the public health system, they are constantly being told "Save money!" "Keep costs down!" "Eliminate fraud and waste!" These messages are so ingrained within the system, that the system does not know how to respond to the new needs of COVID.
For instance, some health care providers think it would be a great idea to send moderate risk COVID patients home with a low cost pulse oximeter so that if oxygen saturation drops around day 8--like they do for those who go on to die--the patient knows to come back and maybe have a fighting chance. However the system that counts the money says "No way!" And then justifies its budget based decision by saying something like "If they read the oximeter wrong then they may come back to the ER unnecessarily and tie up services and put themselves at risk". (At risk of what, I have to ask? They already have COVID.)
Is not it better for someone to present to the ER with a false emergency rather than die at home for lack of info that would be readily available with an oxygen meter that the poor cannot afford but a health care system could buy in bulk and distribute? The answer, if you are a public health bean counter is a resounding "No."
Then there is personal protective gear, aka PPE. We have all seen the doctors and nurses in New York running around in a single (non N95 mask) with no other protective gear. And we have seen them die. Well, it is happening all across the country in public (i.e. "free" ) clinics. If you work at a for profit hospital and work around potential COVID patients, you will get this

If you work for public (non profit) health you will get this

And will be told "If they do not have symptoms then they can't have COVID and you are not at risk." Yeah. Right. Never mind that some people who have COVID have been proven to be contagious without symptoms. Never mind that simply speaking certain consonants can mobilize as many respiratory particles as a cough. Never mind that you can catch COVID through the eyes (or the openings on the side of that flimsy mask).
The safe way to get up close and personal with patients during a time when we are supposed to self isolate due to anyone could have COVID looks like this
 ?width=540&height=&fit=bounds&auto=webp
?width=540&height=&fit=bounds&auto=webp
Or maybe this
 ?itok=TNbHy3NI
?itok=TNbHy3NI
But these items are in short supply, FEMA keeps confiscating them and the Trump family keeps jacking up the price. Since the public health system cannot stop working, those who direct the public health system utter a string of lies about why such PPE is not needed in the public health sector (though apparently it is needed in the private health sector) and tell their front line health care providers "You are just being a bunch of whiny babies. You won't catch COVID. Get back to work."
How much time and money has gone into training the doctors, nurses, respiratory therapists who are going to get sick and die? How will we replace them? This is why I call these "cost saving measures" Penny wise and pound foolish. I guess the bean counters figure they will snatch up some low risk medical students to replace the 50 and 60 something nurses and doctors who are sacrificed on the altar of "fiscal accountability".
No one is listening to the providers. So, maybe we need to have the patients speak up. If you go to a public health clinic and see that the employees have a single flimsy paper mask even though they are getting exposed to sputum particles, maybe you should speak up. These health care providers have made a decision to take jobs that pay less and require more work. They are putting their lives on the line for you. Let them know you care.
Need a plan to save our right to vote this fall.
Wisconsin should be a wake up call to us all. The SCOTUS intervened and as a result there were 5 polling places in a Democratic stronghold that usually has 100.People stood outdoors, exposing themselves to COVID for hours in order to exercise their rights. And Trump says he likes it that way, because the suppressed Democratic/urban voter turn out gives his party a chance to win this fall.
Trump's outlaw wannabe supporters would like nothing better than to see him close urban polling places the way they were closed in Wisconsin, limit absentee and mail voting and make voter turn out low, low, low this fall. Since the MAGATs love Trump because he is a criminal who gets away with it and because they see him as the Godfather of white privilege (stealing the labor of everyone else to line white folks' pockets the way the Yakuza and Mafia steal other folks' labor), they will not be swayed by talk of the law or fairness. They want things to be criminal. And the Supreme Court of the United States has one mandate---suppress the vote.
So, Democrats, time to play hardball. No spending bill gets out of Congress unless it includes provisions to enable voting this fall. If the Red States suffer from lack of stimulus money, they will suddenly put immediate self interest before dreams of pie in the sky by and by return to the day of Jim Crow when every white man was king even if all he did all day was sit on his ass.
And House, you need to launch inquiries (and lawsuits if necessary) to thwart Trump's attempts to line his own pockets with the stimulus money and "reward" his faithful Red State MAGATS with pork that they do not need. Because in addition to grifting, he also plans to make it clear to his loyal base that if they support him for another term as Godfather, he will make them rich. A lie, of course, but these poor fools will believe anything.
Some Doctors Do Not Know How to Read (More on Scary Steroids)
Was told today by the same urgent care that has prescribed short courses of steroids for my asthma for years that they no longer use oral steroids to treat asthma exacerbation. Because of COVID.
WTF!
Here is the WHO position paper that is causing all the controversy. Note that the paper says do not give steroids routinely for COVID due to lack of proven efficacy and possible (not proven) harm.
https://apps.who.int/iris/bitstream/handle/10665/331446/WHO-2019-nCoV-clinical-2020.4-eng.pdf
Some doctors are treating this as dogma. An 11th Commandment. Thou Shalt Not prescribe Oral Steroids for Anyone in a COVID Pandemic. If they would just read the fine print they would see that the WHO also says
Given the lack of effectiveness and possible harm, routine corticosteroids
should be avoided unless they are indicated for another reason. Other reasons may include exacerbation of asthma or COPD,
septic shock, and risk and benefit analysis needs to be conducted for individual patients.
See that, Urgent Care! Asthma is still considered a reason for Prednisone. Unless you own a chain of hospitals and want to put all the asthmatics into them. Early short course steroids have been proven to improve asthma and cut down the risk of hospitalization. If you wait too long , then it takes even longer for the asthma to get better.
Here is the American Academy of Allergy Asthma and Immunology weighing in:
There have been several reports that steroids are contraindicated in COVID-19 disease, so many are wondering what should people with asthma do if their controller medication is a steroid (inhaled or oral). The short answer is continue taking your controller medications and do not stop them. The data suggesting that steroids might increase the shedding of SARS-CoV-2 comes from treating hospitalized patients with systemic steroids just for the viral illness. The use of steroids for treating other diseases (like asthma) was not studied. However, people with asthma are placed on controller medications to keep their asthma under control. In the current pandemic, the best thing a person with asthma can do (with respect to asthma) is to get and keep their asthma under control. Stopping a controller medication will put the person at risk for developing an asthma exacerbation—especially as we enter spring allergy season. In the current pandemic, treatment of an exacerbation will likely require going to the emergency department or urgent care, where the individual has a much higher risk of being exposed to someone with COVID-19. So, in a way, by continuing to keep asthma under control, the person with asthma is actually reducing their chance of exposure to COVID-19.
https://www.aaaai.org/conditions-and-treatments/library/asthma-library/covid-asthma
I was able to avoid the ER. I went to another Urgent Care, luckily a doctor I knew was working and I scored some Prednisone (gasp!) along with inhalers.
It is a hard, cruel world out there right now for asthmatics and COPDers.
Time for Young People to Step up and VOTE in 2020
Generally, young voters in our country our under represented in elections. This could be the year that all changes.
WASHINGTON — State officials nationwide are scrambling to adjust to stay-at-home and social distancing orders as they plan the 2020 voting calendar, and many experts warn that the pandemic threatens to be highly disruptive to this year's elections.
"There's a real possibility that people will be afraid to vote on Election Day and won't have alternatives," said Trevor Potter, a former chairman of the Federal Elections Commission who now heads the Campaign Legal Center in Washington. "That's just unacceptable for the world's leading democracy."
https://www.nbcnews.com/politics/2020-election/election-chaos-coronavirus-fear-voting-could-keep-people-polls-n1174416
The obvious solution is mail in voting. However it is extremely unlikely that Moscow Mitch and Resident Trump will allow this. Their dream is an election in which urban voters stay home for fear of COVID 19, leaving only the deep rural voters.
I would like to propose another solution. Register and get out the vote of the nation's twenty-somethings. Yes, we know that a few people in that age group will have complications from COVID. However, their risks are much lower than that of their grandparents, the elderly who can generally be counted upon to vote in every election.
The future is now. This election will determine the fate of our country. We cannot survive another pandemic in which Trump fiddles while Jarrad Kushner sells off our supplies to the highest bidder. We cannot survive a world in which there are no jobs except for grocery store stockers. We cannot survive a world in which treatable disease will kill you because our health care system is stretched to the max.
If you are one of the lucky young healthy Americans with a long future before you, seize that future. Make it yours.
Public Enemy Number One During COVID 19
So, when Trump said we have shortages because some folks are pilfering supplies, do you think he was referring to this man?

"You also have a situation where in some states FEMA allocated ventilators to the states, and you have instances where in cities they're running out but the state still has a stockpile. And the notion of the federal stockpile was it's supposed to be our stockpile — it's not supposed to be state stockpiles that they then use," Kushner said.
Has anyone considered reusable PPE?
I am old enough to remember when surgical gowns were made of cotton. They were specially washed them sealed and opened when needed. Same for surgical instruments. Same for many of the things that are now made out paper/plastic and cheap metal. And this was in the operating room where materials must be absolutely sterile.
When dealing with COVID, the barrier function is most important. And then you need to be able to decontaminate the PPE so it can be used again.
Why not have cotton gowns? What about face masks made of something besides paper? What about face shields with scratch resistant/shatter resistant glass? Have you seen how quickly the trash bag fills up in just one COVID room? Health care personal entering and then leaving, even if only for a moment, must shed their gear. There are not enough trees in Southeast Asian and the Amazon to make enough gowns for everyone in the world who will eventually get this infection.
Some American Doctor are Now Treating Steroids Like Medical Malpractice Even for Non COVID Disorders
Not kidding. Know a couple of asthmatics who know that they require a short course of steroids to keep them out of the hospital who can not get steroids due to "Everyone knows" that steroids in COVID will kill you. I have heard this twice in the past week so I decided to investigate to see where is this general wisdom coming from.
It isn't coming from this study in China:
https://www.medrxiv.org/content/10.1101/2020.03.06.20032342v1
Critique:This was a retrospective study not a prospective study. Possible reason for not using steroids---only one major contraindication uncontrolled diabetes. Since uncontrolled diabetes makes every infection worse, maybe the group that did not get steroids had an extra strike against them and the steroids for the other group did not do anything. On the plus side these were all classified as severe meaning the authors did not compare oranges to apples.
https://apps.who.int/iris/bitstream/handle/10665/331446/WHO-2019-nCoV-clinical-2020.4-eng.pdf
OK ,here are some recent guidelines for COVID management. Note that the findings are based upon studies of SARS and MERS and Influenza, not COVID. Note that these are observational studies--that means they looked at people who were selected to receive steroids and compared them to those who were not. Now, image that a steroid dependent asthmatic got SARS. Yes, of course they would have gotten steroids. Lots of steroids? Could their underlying lung disease have led to a worse outcome? You tell me. The studies listed below do not.:
survival benefit and possible harms (avascular necrosis, psychosis, diabetes, and delayed viral clearance) (62). A systematic
review of observational studies in influenza found a higher risk of mortality and secondary infections with corticosteroids; the
evidence was judged as very low to low quality due to confounding by indication (63). A subsequent study that addressed this
limitation by adjusting for time-varying confounders found no effect on mortality (64). Finally, a recent study of patients receiving
corticosteroids for MERS used a similar statistical approach and found no effect of corticosteroids on mortality but delayed lower
respiratory tract (LRT) clearance of MERS-CoV (65). Given the lack of effectiveness and possible harm, routine corticosteroids
should be avoided unless they are indicated for another reason. Other reasons may include exacerbation of asthma or COPD,
septic shock, and risk and benefit analysis needs to be conducted for individual patients.
Here is the conclusion of study 62 above:
https://www.ncbi.nlm.nih.gov/pubmed/16968120
CONCLUSIONS:
Despite an extensive literature reporting on SARS treatments, it was not possible to determine whether treatments benefited patients during the SARS outbreak. Some may have been harmful. Clinical trials should be designed to validate a standard protocol for dosage and timing, and to accrue data in real time during future outbreaks to monitor specific adverse effects and help inform treatment.
25 inconclusive and 4 possible harm adds up to be inconclusive, not definitely will kill you.
Maybe the evidence in the next study is more compelling
Here is citation 63
https://www.ncbi.nlm.nih.gov/pubmed/26950335
We did not identify any completed RCTs of adjunctive corticosteroid therapy for treating influenza. The available evidence from observational studies is of very low quality with confounding by indication a major potential concern. Although we found that adjunctive corticosteroid therapy was associated with increased mortality, this result should be interpreted with caution. In the context of clinical trials of adjunctive corticosteroid therapy in sepsis and pneumonia that report improved outcomes, including decreased mortality, more high-quality research is needed (both RCTs and observational studies). Currently, we do not have sufficient evidence in this review to determine the effectiveness of corticosteroids for patients with influenza.
That is not compelling at all.
Moving on to 64.
https://www.ncbi.nlm.nih.gov/pubmed/27036638
Corticosteroids were commonly prescribed for H1N1pdm09-related critical illness. Adjusting for only baseline between-group differences suggested a significant increased risk of death associated with corticosteroids. However, after adjusting for time-dependent differences, we found no significant association between corticosteroids and mortality. These findings highlight the challenges and importance in adjusting for baseline and time-dependent confounders when estimating clinical effects of treatments using observational studies.
Hmm. So, depending upon which line you read, steroids either kill you--or they don't.
Citation 65
https://www.ncbi.nlm.nih.gov/pubmed/29161116
Corticosteroid therapy in patients with MERS was not associated with a difference in mortality after adjustment for time-varying confounders but was associated with delayed MERS coronavirus RNA clearance. These findings highlight the challenges and importance of adjusting for baseline and time-varying confounders when estimating clinical effects of treatments using observational studies.
And then 66 a paper reviewing the use of steroids for sepsis
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6083439/
Two new trials of corticosteroid treatment for sepsis came to differing conclusions
Corticosteroids may reduce the risk of death by a small amount and increase neuromuscular weakness by a small amount, but the evidence is not definitive
This guideline makes a weak recommendation for corticosteroids in patients with sepsis; both steroids and no steroids are reasonable management options
More (not) compelling evidence
https://jamanetwork.com/journals/jama/article-abstract/2763879
Here the Lancet sums up all the ways that steroids with COVID will (not) kill you:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)30317-2/fulltext
The word that jumped out at me was "survivor". I would much rather have a steroid side effect and be alive than die with strong bones.
It is going to be close to impossible to do a study about the risk/benefits of steroids for COVID. Those who are already on steroids when they get sick are likely to have asthma or be immune suppressed--increasing their risk for severe disease.
But please, can we stop punishing those who actually need their steroids to breathe by saying "In this climate, I am not prescribing steroids"? It makes it sound like health care providers are more concerned about not getting sued than about treating individual patients for their individual needs.
Can We Keep Giving Our Nation's Veterans the Respect They Deserve?
Little bit surprised to see a thread about how our veterans are over rated climbing up the charts at DU just as the National Guard is being called out to fight COVID.
There are many reasons to respect our veterans.
Being in the military service means giving up your civil rights. Freedom of speech? Not happening. It might jeopardize national security.
OSHA and a safe workplace? That is strictly "Need to know." If it makes our nation's security even one iota weaker in the eyes of even one military expert you will never find out what chemicals you were exposed to when you served.
Mother-child bond? Father-child bond? Fiance-fiance bond? Country comes first.
If your superior officer tells you to push the button and launch the bomb, you do not get to try to decide how many innocent children might be hit. You are expected to do your job. Imagine the kind of moral crisis that can cause.
Not to mention if you are told "You are on point" you cannot contact your union rep and say "But I need better gear." If you showers electrocute you, then your only option is not to shower. If you are stationed in a country where you allies sexual harass and even rape you, you are expected to keep your mouth shut for the greater safety and good of the military alliance.
People who sign up to serve and who compete their services and get an honorable discharge have made sacrifices that most Americans would never be able to make. How many of you out there would be willing to let someone else make all your decisions for you? Where you sleep, what you eat, how your train? How many would allow yourself to be stationed in some of the most dangerous places on earth?
There are very good reasons why the usual laws do not apply when it comes to war. War is not the natural state of a society. All the rules are upended. And the people who serve are like Alice thrust into a very dangerous Wonderland. They did it for you and me, so we would not have to.

Sleep (yes) and Melatonin (maybe) to Balance the Immune System
Since I am a physician who also has a Masters Public Health, I am going to try to keep up with the article showing up in journals and also try to analyze them in a way that folks without this training may find useful. I am not advocating any particular treatments (unless a prospective double blind trial shows good results and there will be no prospective double blind trials coming out in the next few weeks on COVID because it is just not possible to do them)
The article below is a discussion rather than the results of a clinical trial but it is worth reading especially if you consider the natural course of melatonin production in humans is a graph that looks like this:
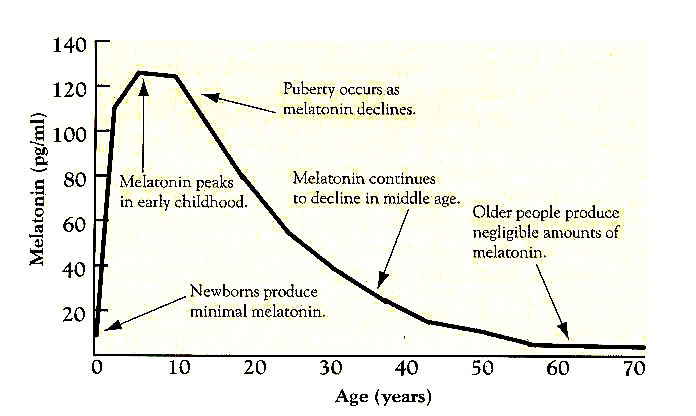
Here is the article:
https://www.sciencedirect.com/science/article/pii/S0024320520303313
Here is the abstract:
This article summarizes the likely benefits of melatonin in the attenuation of COVID-19 based on its putative pathogenesis. The recent outbreak of COVID-19 has become a pandemic with tens of thousands of infected patients. Based on clinical features, pathology, the pathogenesis of acute respiratory disorder induced by either highly homogenous coronaviruses or other pathogens, the evidence suggests that excessive inflammation, oxidation, and an exaggerated immune response very likely contribute to COVID-19 pathology. This leads to a cytokine storm and subsequent progression to acute lung injury (ALI)/acute respiratory distress syndrome (ARDS) and often death. Melatonin, a well-known anti-inflammatory and anti-oxidative molecule, is protective against ALI/ARDS caused by viral and other pathogens. Melatonin is effective in critical care patients by reducing vessel permeability, anxiety, sedation use, and improving sleeping quality, which might also be beneficial for better clinical outcomes for COVID-19 patients. Notably, melatonin has a high safety profile. There is significant data showing that melatonin limits virus-related diseases and would also likely be beneficial in COVID-19 patients. Additional experiments and clinical studies are required to confirm this speculation.
This is not a study result. However if you read through the text there are some interesting points made about how melatonin has been shown to reduce CNS and nerve damage in lab rats given certain viral infections. And COVID appears to be an RNA virus that affects the central nervous system via the olfactory nerve which is adjacent to the nose and therefore a site where viruses can easily enter the brain.
There are also human studies showing that melatonin may decrease the level of cytokines and inflammation in people with other disease.
Although there is obviously no report related to the use of melatonin in COVID-19 patients, in subjects with other diseases and an increased level of inflammation, the application of melatonin showed promising results regarding the attenuation of circulating cytokines levels. In a randomized controlled trial, 8-week oral intake of 6 mg/d melatonin caused a significant decrease in serum levels of IL-6, TNF-? and hs-C-reactive protein (hs-CRP) in patients with diabetes mellitus and periodontitis [56]. In another trial of patients suffering with severe multiple sclerosis, orally 25 mg/d of melatonin for 6 months also promoted a significant reduction in serum concentrations of TNF-?, IL-6, IL-1? and lipoperoxides [57]. In the acute phase of inflammation, including during surgical stress [58], brain reperfusion [59], and coronary artery reperfusion [60], melatonin intake of 10 mg/d, 6 mg/d and 5 mg/d of melatonin for less than 5 days induced a reduced level of pro-inflammatory cytokines. A recent meta-analysis of a total of 22 randomized controlled trials suggested that a supplementary use of melatonin is associated with a significant reduction of TNF-? and IL-6 level [61]. This clinical evidence suggests that the use of melatonin as a supplement may effectively reduce the levels of circulating cytokines, and may potentially also lower pro-inflammatory cytokine levels in COVID-19 patients.
This goes along with something I have been thinking. Youth does not necessarily protect us from new viruses. A disproportionate number of young people died from the 1918 flu pandemic.
https://www.sciencedirect.com/science/article/abs/pii/S0022519311003894
However something appears to be protecting younger people from COVID 19's worst effects. Could it be a hormone that is present in higher levels in young people? Might not be melatonin. There are many hormones that vary by age.
Note that the doses used in the human test above are not huge. 3 mg, 5 mg, 10 mg. These are the usual recommended doses for normal function. The goal is not to kill the virus with melatonin. The goal is to achieve a pattern of sleep (which affects on the immune system) as much like that as a young person as possible. You are looking for normal.
Along these same lines, sleep hygiene--getting enough rest at the same time every day while limiting things which can affect sleep architecture (like alcohol and stimulants before bedtime) limiting things that can cause you to reflux in your sleep (like eating before bedtime, lying down flat on your back after eating) and using your sleep apnea treatment might also bolster the immune system.
Had to search long and hard for a review of sleep and in the immune system that is not behind a pay for view wall. Thank you NCBI (National Center for Biotechnology Information) for sharing this one.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3645929/
Inflammation modulates sleep and the effects of sleep loss and conversely sleep or sleep loss alters inflammatory responses including the production of inflammation regulatory substances activated by neuronal/glial use and immunologic pathogen recognition
PS: For those that want advanced reading, this is a fascinating study about how RNA viruses (like COVID) work in the immune system. Notice that some of them have a biphasic pattern. They do one thing in the initial infection and then later act differently. Full PDF available thanks to ncbi
https://www.annualreviews.org/doi/abs/10.1146/annurev.mi.40.100186.001111
Profile Information
Member since: Tue Nov 9, 2004, 07:05 PMNumber of posts: 19,240