2016 Postmortem
Related: About this forumMisconceptions about health care.
In discussing healthcare and single payer recently, I've come across a couple persistent misconceptions, so I decided to write an OP to correct these.
Misconception #1: the rest of the developed world has single payer. I'm not sure why this belief is so widespread, but it is very far from the truth. It's true that the rest of the developed world has universal coverage. But universal coverage and single payer are very different things. Here's a list of countries providing universal coverage and how they provide it.
http://truecostblog.com/2009/08/09/countries-with-universal-healthcare-by-date/
There are basically three methods.
--Single payer, where the government covers it all. Canada is an example.
--Hybrid systems, where a single payer covers basic care, and private insurance covers the rest. France is an example. According to Wiki 85% of French citizens have private insurance on top of the government coverage. That's very far from medicare-for-all.
--Mandates. This is basically Obamacare -- everyone has to buy insurance, some of it is subsidized, and there is community rating. Holland and Germany are examples of this.
Misconception #2: our system is so expensive because of profits for drug and insurance companies. This is factually wrong, which can be verified by looking up the numbers. The best discussion of why the US system is so expensive I've found (via Krugman's blog) is here.
http://theincidentaleconomist.com/wordpress/what-makes-the-us-health-care-system-so-expensive-introduction/
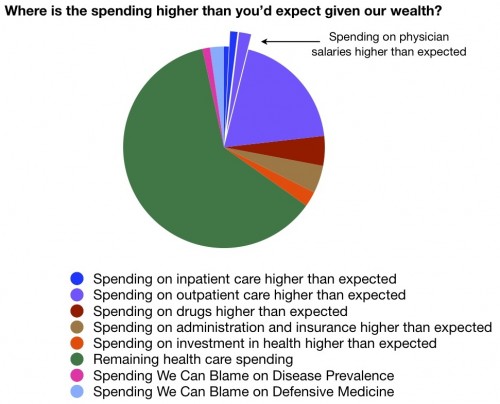
The basic conclusion: everything costs more in the US. There's no one thing that will bring us in line with the rest of the world. Drugs are part of it, so are administrative expenses, but most of it is just that we spend more on care. This chart breaks down our excess spending. The green part is what we would pay if healthcare spending as a fraction of GDP was in line with other countries. The other colors are where we relatively overpay. The bulk of it is outpatient care, and has nothing to do with salaries, drug costs, or insurance administration.
Misconception #3: single payer is the only thing that will fix our system. This is actually two misconceptions in one. The first is that single payer is a silver bullet. And the second is that there are no alternatives. There is no basis for either.
As we've seen, around the world, there are various ways to control costs while providing good universal coverage. International comparisons don't support the single-payer-or-bust theory at all.
Within the US, the big appeals of single payer are (1) it will reduce administrative overhead and (2) it will reduce prices by giving the government bargaining power. (1) is true, it will be cheaper to administer, but administrative costs are a small part of the problem. (2) is trickier, though.
With single payer, the government can drive a hard bargain by refusing to pay high prices for drugs and treatments, but there's obviously a downside: it means that some things are not going to be covered. It could and probably will mean things like hospital closures. The healthcare delivery system is now organized around a certain price schedule, and changing that will require re-organizing things, which will be disruptive. We would probably come out of it OK, but the transition will not be smooth.
But the thing is, none of that actually requires the government to be doing the paying. It just requires the government to be doing the price-setting. Not even that, in fact. It just requires that providers have to negotiate with everyone at once, instead of carving out special deals with different insurers. There are other ways to achieve this. One is simply for the government to impose price controls. Another, widely discussed, is all-payer rate setting, which simply forces every provider to charge everyone the same price, effectively grouping all consumers into one big block for pricing purposes.
I'm not exactly sure why there is so much insistence on single payer as the only route to universal, reasonably priced coverage. There are other alternatives which are not only politically more feasible, but also logistically more feasible given where we are right now.
 = new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
= new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
ViseGrip
(3,133 posts)
Recursion
(56,582 posts)Many countries have for-profit providers and for-profit insurers.

DanTex
(20,709 posts)In single payer systems, healthcare providers, drug companies, etc. still have a profit motive. It's sort of like when the government hires private contracting companies to build infrastructure projects. The contractors still have a profit motive.
Recursion
(56,582 posts)and it's only gotten worse.
There are as many ways to finance health care as there are countries; and as you point out, financing is not a silver bullet.

daleanime
(17,796 posts)as to think that health care for all would be a good thing?
Just in case.
 Have a lovely day.
Have a lovely day.