2016 Postmortem
Related: About this forumAre you willing for doctors and hospitals to make half of what they make now
while serving 80 million more people than they are now?
Where would you like those cuts to come from? Should physicians' salaries be protected and hospital budgets slashed? (And what about physicians at hospitals?).
Here, per Center for Medicare and Medicaid services, is our national health expenditure data (2014 is the last year they have).
https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/NationalHealthExpendData/Downloads/Tables.zip
Look in particular at Table 2, "National Health Expenditures; Aggregate, Annual Percent Change, Percent Distribution and Per Capita Amounts, by Type of Expenditure: Selected Calendar Years 1960-2014"
Since people get pissy when I post charts, I'll just list the numbers:
The US spent $3.03 trillion on health care in 2014.
That gets divided into the following:
Hospital Care: $971 Billion
Physician Services: $603 Billion
Other Professional Services: $84 Billion
Dental Services: $113 Billion
Home Health Care: $83 Billion
Nursing Care: $155 Billion
Pharmaceuticals: $297 Billion
Durable Medical Equipment: $46 Billion
Consumable Medical Equipment: $57 Billion
Government Overhead: $40 Billion
Private Insurance Overhead and Profit: $195 Billion
Public Health: $79 Billion
R&D: $45.5 Billion
Structures: $108 Billion
If we want to cut our health care spending in half, to get down to the levels that other countries spend, we have to cut $1.5 Trillion from that. (EDIT -- Sanders wants to get it down to $1.3 Trillion, so you have to cut $1.7 Trillion to get there.)
Remove all private insurance overhead and that leaves $1.3 Trillion.
Find it. Go ahead. Where do you want that $1.3 Trillion to come from? Hospitals and Doctors are the only big juicy targets there, along to a lesser extent with Pharma.
Let's say Pharma magically operated for free in the US, and let's say government insurance magically had no overhead (we already eliminated private insurance overhead above). That cuts $340 Billion, which means we have to find slightly less than $1 Trillion to cut still, and the only places that still look big enough to have much of an impact there are Hospitals and Physician Services. $1 Trillion would mean cutting their reimbursement by two thirds, which we all know we can't do, so we'd have to find some money elsewhere (structures? public health? dentists?).
Worse still, 80 million Americans or so skip at least some needed medical care right now because of cost (30 million are uninsured; the rest cannot afford to use their insurance).
This means we're trying to pry $1 Trillion mostly out of doctors and hospitals, while asking them to treat 80 million more people.
If you don't want most of that $1 Trillion to come from doctors or hospitals (remember we're already pretending drugs are completely free and financing has zero overhead), where do you want it to come from?
(BTW, I am; I'm just curious if people are really aware of how big the cuts we're talking about are. I'll go back on my no-chart pledge to post one I posted downthread:

That's a pretty big gap.)
 = new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies
= new reply since forum marked as read
Highlight:
NoneDon't highlight anything
5 newestHighlight 5 most recent replies

CaliforniaPeggy
(149,525 posts)That's my question.

Recursion
(56,582 posts)The OECD average for physicians is much lower than for the US:
(And that chart is just for GPs; specialists in the US really skew the numbers up.)
And for-profit hospitals are essentially unknown.
ViseGrip
(3,133 posts)I think not....
Recursion
(56,582 posts)Remember that French couple he has dinner with? I was really glad that Moore did in fact focus on the need for provider reform in addition to finance reform, even though a lot of his fans seem to have skipped that part.

kristopher
(29,798 posts)"Finance reform" as you misleadingly call it, is the key to cost reductions in all areas. Virtually every facet of medical care is supported in pricing by some sort of cartel like mechanism. The only way those cartels can be defanged is to go to a "Single payer" model where the medical community becomes price takers instead of price setters.
But you already know that.
Recursion
(56,582 posts)Which rows does the $1.7 Trillion Sanders is claiming we will save come from.
kristopher
(29,798 posts)Recursion
(56,582 posts)In 2014, the median weekly earnings of Americans with advanced degrees was $1386, which translates to $72,000, or about what physicians make in Sweden.
kristopher
(29,798 posts)The 5 person sample of primary providers I've asked about this is small, but those who are in it to actually practice medicine are thrilled with the idea of single payer. They HATE running a business.
Then there are those who see the opportunity for squeezing profits out of every facet and phase of heath care provision. For example, they decide that they need an extremely expensive piece of equipment not because the benefit can't be obtained locally from an other equipment owner, but because they deem ownership to be a profit opportunity that can be enhanced by inserting a new level of "caution" into their procedures.
In fact, a large part of our infrastructure is almost certainly dramatically under utilized. Of course, tightening down the screws will inevitably lead to shortages. But, that is the balancing act which is required; it has to be dynamic in order to have the system operate in the desired area of minimum cost/maximum benefit.
Recursion
(56,582 posts)
passiveporcupine
(8,175 posts)Doctors group welcomes national debate on ‘Medicare for All’
Reality: Single payer is the only health reform that pays for itself. By replacing hundreds of insurers and thousands of different private health plans, each with their own marketing, enrollment, billing, utilization review, actuary and other departments, with a single, streamlined, tax-financed nonprofit program, more than $400 billion in health spending would be freed up to guarantee coverage to all of the 30 million people who are currently uninsured and to upgrade the coverage of everyone else, including the tens of millions who are underinsured. Co-pays and deductibles, which have been rapidly rising under the Affordable Care Act, would be eliminated. Further, the single-payer system’s bargaining clout would rein in rising costs for drugs and medical supplies. Lump-sum budgets for hospitals and capital planning would control costs even more.
A single-payer system would also greatly diminish the administrative burden on our nation’s physicians and hospitals, freeing up physicians, in particular, to concentrate on doing what they know best: caring for patients.
http://www.democraticunderground.com/12511080467
http://www.pnhp.org/news/2016/january/doctors-group-welcomes-national-debate-on-%E2%80%98medicare-for-all%E2%80%99
I've not read it all yet, but I don't think all these doctors would be for single payer if they thought it was going to break them financially.
Recursion
(56,582 posts)Which I posted in that thread.
kristopher
(29,798 posts)Recursion
(56,582 posts)
1939
(1,683 posts)for a BS in Electrical Engineering to a BA in Theater and Drama.
Recursion
(56,582 posts)And even more oddly, the most common job right now among both sets of classmates is "IP Lawyer".
kristopher
(29,798 posts)I hoped to offer a starting point for discussion. You've raised the second step - comparisons within that basic group.
But let me first put a small curve in the road - is an ethicist with a philosophy background worth more, the same or less than a family physician?
What about a lawyer?
Does a Corporate CEO or a hedge fund manager "deserve" to make hundreds of millions per year?
How much is a hospital administrator worth?
How much is a solder who gives his/her life to defend the country worth?
How about a taxi driver or a fisherman who is killed while working?
How is "worth" measured?
Are medical doctors paid more than they "should" be because the AMA artificially constrains the supply of medical doctors?
What I'm really getting at, is how do we divide the resource pie up among us all?
It is pretty much a zero sum game. So, while the relative value of each of us certainly differs depending on many factors, isn't there a place to start where the idea is we all have a basic "worth" by virtue of being a part of a civil society?
passiveporcupine
(8,175 posts)So, while the relative value of each of us certainly differs depending on many factors, isn't there a place to start where the idea is we all have a basic "worth" by virtue of being a part of a civil society?
A lot of people have gotten into the medical field (and dental and legal) for one reason. It pays much better than most other fields. They are in it for the money, primarily.
Is profit really what we want to drive our citizens into the field of medicine?
Banking didn't used to be what wall street is today. Everything evolves and not always for the better.
This country has been so driven by capitalism and profit and the idea of becoming "wealthy" that it no longer takes into account the value of the human being in all of us.
cannabis_flower
(3,764 posts)The doctors in Sicko didn't make as much but still enough to drive a luxury car, live in an expensive house, send their kids to private school and have nice vacations. What more do they want?

whathehell
(29,034 posts)made about 200k and that was seven or eight years ago...Little to no difference to average early career salaries of doctors here.
Recursion
(56,582 posts)Which is $65K or so in USD.
whathehell
(29,034 posts)and what averages are you talking about? Are you saying French physicians are making LESS today?
Recursion
(56,582 posts)And I remember Moore talking with a French woman I thought was a doctor.
whathehell
(29,034 posts)and seven/eifght years ago it was worth more.
lumberjack_jeff
(33,224 posts)Further, their work week is 35 hours, they have a dozen paid national holidays, and every worker has at least 5 weeks of paid leave.
http://www.cbsnews.com/news/france-less-work-more-time-off/

boobooday
(7,869 posts)And are not burdened with hundreds of thousands in student loans.

SusanCalvin
(6,592 posts)Only question is how to get there. If other countries can do it, so can we.

FourScore
(9,704 posts)
and that chart is from almost 10 years ago.
The whole post is rather uninformed, as it excludes so many areas of the health industry:

Recursion
(56,582 posts)Is Center for Medicare and Medicaid Services just wrong?
I also rolled up all of the devices into one category (because CMS does) and all pharma into one category. Their margins are high but their size is miniscule compared to medical services.
passiveporcupine
(8,175 posts)The cost of health care will go down much more than your numbers are predicting if insurance and processing is reduced to one system for all doctors and patients. Doctors won't need huge offices full of staff to handle just the insurance processing.
From the PNHP group you dismissed:
with a single, streamlined, tax-financed nonprofit program, more than $400 billion in health spending would be freed up to guarantee coverage to all of the 30 million people who are currently uninsured and to upgrade the coverage of everyone else
Your chart lists overhead and profit for the insurance companies, but doesn't touch the cost of doctors/hospitals to have sufficient staff to handle all those insurance policies. You are not seeing the whole picture. Just what they want you to see, which is why statistics can always be used in anyone's favor.
Recursion
(56,582 posts)What about the remaining $800B?
passiveporcupine
(8,175 posts)That is just one of the things they are pointing out as a real savings.
whathehell
(29,034 posts)
Jarqui
(10,122 posts)How about they take a cut in pay until they change that result because I don't have confidence the US is paying the most and getting the best when folks are not living as long.
Regardless, they could still take a cut in pay and make the most in the world. If they take a cut in pay and are still the top paid physicians in the world, where are they going to go to get more money?
Here's an interesting thought:
From above: "Physician Services: $603 Billion"
US GP physicians above could get $125,000 (24% cut down from $165,000) and still be the top paid in the world. (yes, I know they'd howl).
24% cut on $603 Billion is $146 billion = pretty close to what we'd need to cover the 29,000,000 who don't have healthcare with 0.1% of them dying each year because the lack coverage.
See how that might work?
I don't think they need to chop 50% or anywhere close to that. But there's plenty of fat in the system they can cut while the doctors can still be the top paid and the services are top notch for everyone.
Recursion
(56,582 posts)Jarqui
(10,122 posts)0.1% of 29,000,000 = 29,000 of those without healthcare die annually.
I'd take my chances on mortality during a doctor's strike every five-ten years over losing 29,000 a year that we'll continue to lose under the current mess.
Several articles report something like this:
http://www.ncbi.nlm.nih.gov/pubmed/18849101
The articles analyzed five strikes around the world, all between 1976 and 2003. The strikes lasted between nine days and seventeen weeks. All reported that mortality either stayed the same or decreased during, and in some cases, after the strike. None found that mortality increased during the weeks of the strikes compared to other time periods.
So it's not like a nasty epidemic of death breaks out when they go on strike.
Recursion
(56,582 posts)Sorry, I was saying that when doctors go on strike slightly fewer people die.
wilt the stilt
(4,528 posts)As a nation we are fat as pigs. We eat terribly, have high blood pressure and diabetes. Current Doctors took on way bigger debt than anyone else to get through school. How do you ask them to take a pay cut and survive?
You would have to reform the entire school system.
Jarqui
(10,122 posts)dying prematurely because they do not have healthcare coverage (from 2009 Harvard study that claimed ~45,000 died per year when 45 million were uninsured) would factor in?
Do you think people delaying going to see their doctor because of their high deductible factors in? The doctors do.
And while we're at it, guns don't help a lot here, do they?
No question obesity is a significant problem shortening American lives. But it is not the only reason. Deal with the first two items and I think you'll move the needle.
wilt the stilt
(4,528 posts)Look around you. We are fat pigs. Actually, dying prematurely by gunshot wound or uninsured probably reduces the healthcare spend if you think about it. These people do not access the system at all.
Jarqui
(10,122 posts)But it's not the only problem or only reason life expectancy is low.
I'd argue that some of the obese could get their life extended if they don't have to worry about their high deductible and get a stent put in to buy them a few more years. Others could live longer if they could see their doctors sooner or more regularly and not have to worry about cost and get prevent medical help sooner.
People dying because they can't get healthcare or they have high deductibles is a really preventable cause of death. It takes money. When US doctors earn 25% more than anywhere else in the world and health insurance companies make billions more than anywhere else, I don't have a problem going after them and saying "ante up you greedy pricks, people are dying unnecessarily - not because of a disease we can't cure but because you guys are gouging the healthcare system to line your pockets and not taking care of everybody."
For decades, we have had a capitalist kind of "honor" healthcare system. And it's proven that it will not forsake some profits to look after all of the unfortunate or poor voluntarily. So we have to do it for them because this isn't right.
wilt the stilt
(4,528 posts)However doctors make more because the cost of schools are so high so they need to. Secondly,the amount of time they put into being a Doctor is pretty unbelievable. $175K for a GP I personally think is way underpaid.
Jarqui
(10,122 posts)Talking about obesity, the whole healthcare system has that problem. America could get a much better bang for it's healthcare buck and save more lives if a bunch of the healthcare budgets went on a diet. Single payer happens to be a very successful and efficient way of doing that.
Recursion
(56,582 posts)Medicare has been overpaying doctors for almost 20 years, and just made that overpayment permanent
https://www.washingtonpost.com/blogs/wonkblog/post/faq-the-doc-fix/2011/11/22/gIQAnv6wkN_blog.html
Jarqui
(10,122 posts)"we'll opt out" because single payer is it. Where are they going to opt out to? A few could go to private insurance but not all.
Now, it's money so folks will bicker. But around the world in the universal/single payer systems, doctors are tending to patients and life is going on. They have always worked it out.
It will be more painful for the US doctors because their salaries will be under more pressure to come down because they're so much higher than anywhere else.
And that is a part of single payer where they have a hammer to get the healthcare costs under better control because they're the only major game in the country.
It is going to tougher in the US because their fees and salaries are so high. It cannot happen all at once either. It can migrate to more "competitive" or "reasonable" compensation over time.
It is not just healthcare that is at stake here. Americans have to be able to compete in the world economy. To do that, the healthcare costs have to come down. The rest of the country cannot continue to suffer for a few doctors and the health insurance companies that are making 25-50% more than anyone else in the world. At some point, the country can't compete in another industry and more jobs go to China.

Stargazer99
(2,576 posts)needed RX and she was working (too costly to include medical for the lower classes)
Some people don't mind if others die as long as it isn't them
Jarqui
(10,122 posts)I've had a bad last 30 months losing people (most not due to this) but my wounded heart is sensitive to this horrible, needless and senseless tragedy. I cannot comprehend it happening over political bickering when the money is there to stop it.
The Obama town halls in '08 gave me nightmares. Unbelievable suffering for no good reason.
We moved downtown recently. The homeless people. They break your heart. We didn't give presents at Christmas. We gave everything we could to local charities to try to help them. And it doesn't put a nick in the problem.
This is a big issue for me. I will not stop until this kind of pointless dying stops. We have to prevent this from continuing to happen. I think Bernie is the best and probably only chance to do so any time soon.

enid602
(8,594 posts)Yes US doctors make more $$. But they also PAY a lot more in medical malpractice insurance. Want the more universal insurance that other developed countries have? Adopt tort reform. They all have it, save the US. Bernie's voted against tort reform twice.
Recursion
(56,582 posts)In that compensatory damages would basically cease to exist. But, yeah, I think tort reform has at least some role to play here, though less than Republicans say it would (they think that would magically solve everything, when the whole reason I'm writing these long posts is to stress what I am convinced of, that there is no one thing that will magically fix our system).
And, that said, I think patients should have at least some recourse to the courts.
enid602
(8,594 posts)Try suing a doctor in Canada, France, UK etc. Very hard. All other developed countries have spoken. The rights of the majority to healthcare far outweigh the rights of individuals to sue. We dems are in the hands of the ABA (special interest) on this one. If you want to cut health costs in the US, tort reform is essential.
passiveporcupine
(8,175 posts)It's really hard to get a doctor kicked out of the medical profession, and there have been some really bad doctors out there scamming people, treating them unnecessarily for money, and even killing them. These guys need to be sued. It's about the only way they will have their license taken away.
The accidental problems that come up are one thing...gross negligence is another. Doctors should be held accountable for doing their job right and being as careful as is reasonably possible.
I had a surgery performed in the wrong place on my foot, because the doctor that did it was so old he forgot what he was supposed to be doing. I complained to my insurance company and they held a review with other doctors (without me or my surgical consent form) and the docs decided in his favor because what he did was the most common place that surgery was usually performed.
A year later I saw another doc for the same problem he didn't fix and the doc said he was on that review board. He apologized to me because he said the doc was wrong. He operated in the wrong place. He was stunned and embarrassed because it was so obvious what needed to be done.
I didn't sue. I was an emotional mess and depressed and was not up to doing anything like taking someone to court. I never got the problem fixed and I still have serious life altering problems because of my feet. And I'll never have surgery on my feet again. Ever!
And that old doctor kept on practicing. I wonder how many more mistakes he made before he finally became so senile he had to quit. I should have sued. Not for money, but to get his practice ended. But like I said, I was not emotionally able to do that.

azurnoir
(45,850 posts)most MD's in the US these days graduate from med school with anywhere from $500,000 to 1 million in student loan debt, not tp mention the cost of malpractice insurance which has become particularly burdensome for obstetricians, so much so that some have stopped delivering babies
Recursion
(56,582 posts)first off by making undergraduate education debt-free, secondly by forgiving post-graduate education loans to physicians and other health professionals who work in Federally Qualified Health Clinics.
azurnoir
(45,850 posts)Recursion
(56,582 posts)As I've often said, I really like Senator Sanders, but I just think O'Malley has the better policy ideas here.
azurnoir
(45,850 posts)Recursion
(56,582 posts)Am I wrong?
azurnoir
(45,850 posts)
JonLeibowitz
(6,282 posts)
mucifer
(23,484 posts)and are very much willing to say no to people. They don't try to save every premature baby who weighs less than a pound. They don't do CPR and put people on ventilators when they are very elderly with multiple organ failure. 60 Minutes did a good story on it a few years ago:
http://www.cbsnews.com/news/the-cost-of-dying/
Recursion
(56,582 posts)I can't imagine the freak-out if we actually started adopting the standards of care that are common in the rest of the OECD.

Fumesucker
(45,851 posts)It's also why atheists have the least acceptance in American society of any western nation, we literally scare the religious.
http://www.democraticunderground.com/1218222060
Tom Jacobs from Pacific Standard writes that atheists are not well-liked among believers. Derek Beres says that in his conversations with believers, they think atheists are arrogant, while Jacobs says that others believe that non-believers don't have any morals. However, a recent study published in the journal Social Psychological and Personality Science provides a reason for this antagonism: "Among believers, the mere contemplation of atheism can arouse intimations of mortality."
Recursion
(56,582 posts)Now, personally, I am a theist, but I don't believe in an afterlife or any sort of "immortality of the soul", so I guess in that sense my view of death is closer to most atheists'.
Fumesucker
(45,851 posts)The Shadow knows what evil lurks in the hearts of men.

Dyedinthewoolliberal
(15,546 posts)what does another country spend it's medical money on? What is the difference between theirs and your numbers?
Recursion
(56,582 posts)And hospital reimbursements are also much, much lower (though I don't have a chart for that like I do for physicians, see my response to CaliforniaPeggy).
Basically we spend more money on literally every part of our health care system than every other country does, but where it really shows up is hospitals and doctors.

Fawke Em
(11,366 posts)reformist2
(9,841 posts)SusanCalvin
(6,592 posts)Recursion
(56,582 posts)Canada has 2.2 physicians per 1000 people; the US has 2.4. However, Canada has 1.2 GPs per 1000 people, and the US has 0.6.
SusanCalvin
(6,592 posts)
VulgarPoet
(2,872 posts)slipslidingaway
(21,210 posts)our daughter owes over 200K just for med school, without accumulating interest. That is not the case in other countries.

winter is coming
(11,785 posts)slipslidingaway
(21,210 posts)require to cut through the red tape.

And we threw out almost 10K worth of Neupogen, injections to boost the white count after transplant, that was not used because the doctor's office knew that they could get the first approval from the insurance company, but were worried about the second approval.
A total waste.
Someone profited, it was not the patient and not the doctor.
Recursion
(56,582 posts)I mean, sure, compensatory damages would go away (at least largely; maybe time missed from work or something), but are you saying a provision of single payer should be tort reform eliminating (or at least sharply diminishing) punitive damages?
winter is coming
(11,785 posts)the system wouldn't have to be structured to prioritize insurer profit over patient outcome.
Recursion
(56,582 posts)The majority of hospitals, and essentially all physicians' practices, would still be for-profit entities.
winter is coming
(11,785 posts)Recursion
(56,582 posts)Not-for-profit hospitals are free to exist; not-for-profit physician's practices are too (I actually know a doctor who runs one).
1939
(1,683 posts)Because they accept the payments that the US government makes to them for care, they are "agents of the government" and all malpractice claims are pursued through the government claims process. The government would then proceed to sanction or disqualify doctors or hospitals with excessive claims. Legal sharks like John Edwards could go back to defending traffic tickets.
Recursion
(56,582 posts)Forgive loans for (or better yet pay tuition for) doctors who then work for X years in a Federally Qualified Health Clinic, for whatever value of X CMS's quants say we need to do.
slipslidingaway
(21,210 posts)building on a flawed foundation.
AND stop hiding behind Republicans as if they are the only obstructionists, our own party has not been truthful with the people.
Recursion
(56,582 posts)We can't just adopt their financing model and expect their results with our same old provider system.
slipslidingaway
(21,210 posts)NRaleighLiberal
(60,006 posts)Make corporations pay their share - end the loopholes. Meaning top people in these companies have to part with some of their obscene salaries.
Recursion
(56,582 posts)That would just find a way to continue funding our overpriced healthcare system, when I think we should be looking for ways to spend less money more effectively like other countries seem to do.
NRaleighLiberal
(60,006 posts)yet drug prices are obscene. It is amazing what I observed - mismanagement, no leadership, little creativity, progression of medicines with little to no advantage over placebos - and this is Pharma. Add in insurance company waste, hospital waste - I think effective spending means finding efficiency. I could go on and on - but I am so relieved to be retired and away from being so up close and personal to some utterly depressing, demoralizing, disillusioning things.
Uncle Joe
(58,297 posts)Medicare for All Health Care Plan
$1.38 trillion / year
Paid for by a 6.2 percent income-based health care premium paid by employers, a 2.2 percent income-based premium paid by households, progressive income tax rates, taxing capital gains and dividends the same as income from work, limiting tax deductions for the rich, adjusting the estate tax, and savings from health tax expenditures.
$1.39 trillion / year
https://berniesanders.com/issues/how-bernie-pays-for-his-proposals/
What would the nurses say as they're on the front lines of the health care debate?

Noting his issues “align with nurses from top to bottom,” National Nurses United, the nation’s largest organization of nurses, today endorsed Senator Bernie Sanders for President.
“Bernie Sanders has a proven track record of uncompromised activism and advocacy for working people, and a message that resonates with nurses, and, as we have all seen, tens of thousands of people across the country. He can talk about our issues as well as we can talk about our issues. We are proud to stand with him in his candidacy for President today,” said NNU Executive Director RoseAnn DeMoro.
NNU, which represents some 185,000 nurses from California to Florida, including nurses who live in the early caucus and primary states of Iowa, New Hampshire, and Nevada, becomes the first national union to endorse Sanders.
(snip)
“Bernie’s issues align with nurses from top to bottom,” DeMoro continued. Among them – “insisting that healthcare for everyone is a right not a privilege, protecting Social Security and Medicare from those who want to destroy or privatize it and working to expand both, holding Wall Street accountable for the damage it has done to our communities, understanding the threat to public health from the climate crisis, environmental degradation, and the Trans-Pacific Partnership, support for minimum nurse-to-patient ratios for hospital patients, and on and on,” DeMoro said
The NNU Executive Council voted to endorse Sanders. Factors for NNU backing, said DeMoro, included:
Sanders’ long history of support for NNU, nurses and patients,
A 100 percent scorecard on a questionnaire NNU sent to all the Democratic and Republican Presidential candidates,
Overwhelming support for Sanders among NNU members in an internal poll, and
Sanders’ response to issues before the AFL-CIO Executive Council.
NNU, said DeMoro, has adopted a call to “Vote Nurses Values – caring, compassion, community. Nurses take the pulse of America, and have to care for the fallout of every social and economic problem -- malnutrition, homelessness, un-payable medical bills, the stress and mental disorders from joblessness, higher asthma rates, cancer, heart ailments and birth defects from environmental pollution and the climate crisis. Bernie Sanders’s prescriptions best represents the humanity and the values nurses embrace.”
(snip)
http://www.nationalnursesunited.org/press/entry/nurses-endorse-sen.-bernie-sanders-for-president/
Thanks for the thread, Recursion.
Recursion
(56,582 posts)Which of those rows go down under this plan? Cocktail napkin is fine.
Uncle Joe
(58,297 posts)Recursion
(56,582 posts)And Medicaid provides essentially all of "Nursing Care".
Uncle Joe
(58,297 posts)Recursion
(56,582 posts)"National Health Expenditures by Source of Funds and Type of Expenditures: Calendar Years 2008-2014"
(There are several small "other" and "misc" payment categories that I'm leaving out, so these won't add exactly up to the numbers in the OP)
All dollar amounts are in Billions, so that I don't have to keep typing the word "Billion".
Total gross spending (including overhead & profit):
Out of Pocket: $330
Private Insurance: $991
Medicare: $618
Medicaid: $495
Total non-overhead expenditures:
Out of Pocket: $330
Private Insurance: $869
Medicare: $580
Medicaid: $445
Hospital Care:
Out of Pocket: $31
Private Insurance: $362
Medicare: $250
Medicaid: $168
Physician Services:
Out of Pocket: $54
Private Insurance: $254
Medicare: $138
Medicaid: $64
Other Professional Services:
Out of Pocket: $21
Private Insurance: $30
Medicare: $20
Medicaid: $6
Dentists:
Out of Pocket: $45
Private Insurance: $54
Medicare: < $1
Medicaid: $10
Home Health Care:
Out of Pocket: $7
Private Insurance: $8
Medicare: $35
Medicaid: $30
Nursing Care:
Out of Pocket: $41
Private Insurance: $13
Medicare: $36
Medicaid: $50
(turns out that's got a more diverse payment stream than I thought...)
Pharmaceuticals:
Out of Pocket: $45
Private Insurance: $127
Medicare: $86
Medicaid: $27
Durable Equipment:
Out of Pocket: $23
Private Insurance: $8
Medicare: $7
Medicaid: $6
(Apparently most people buy their own wheelchairs)
Consumable Equipment:
Out of Pocket: $54
Private Insurance: $0
Medicare: $2.3
Medicaid: $0
Uncle Joe
(58,297 posts)those costs be reduced?
Recursion
(56,582 posts)The average spending per person would go down, probably, sure, but those absolute costs would go up.
Uncle Joe
(58,297 posts)national total health care spending?
Recursion
(56,582 posts)The costs per person to Medicare would go down, definitely, but that doesn't necessarily mean absolute total costs would go down (though they probably would, somewhat, which again means doctors and hospitals would make less).
Two factors of everyone going on Medicare would drive total costs down:
1. Medicare pays doctors and hospitals somewhat less than private insurance, in most cases
2. Medicare has lower overhead than private insurance
One factor of everyone going on Medicare would drive total costs up:
3. Everyone would have access to care, meaning the 80 million people who are skipping treatments for cost reasons would stop doing so
#3 is a good thing. A great thing, even. However, it also means that literally 25% of the population would start going to doctors and hospitals much more than they are now, which means doctors' and hospitals workloads would increase by something like one third. (Do we even have enough doctors, for that matter, to do that?)
If the doctors and hospitals are being reimbursed for those people at the same rate they are for currently-insured people, total costs go up.
Uncle Joe
(58,297 posts)go a long way in moving that endeavor along.
Everyone skipping treatments also contributes to lower costs, as an ounce of prevention is worth a pound of cure.
As of today 33 million Americans still aren't insured many of them don't go to a hospital until they end up in emergency room and that adds to hospital costs, millions of others are under insured and the same dynamic plays out.
As I posted above the Nurses are on the front line of healthcare, they do the lion's share of the work why do you believe they endorsed Bernie and his Medicare for all plan?
Recursion
(56,582 posts)Specifically, student loans would be forgiven for doctors who work in a Federally Qualified Health Clinic in an underserved area. That's a great idea.
why do you believe they endorsed Bernie and his Medicare for all plan?
Well, like I said upthread, I also would endorse a plan that gave a Federal guarantee to my revenues, and allowed me to attack anyone trying to reduce them as "cutting Medicare".
Uncle Joe
(58,297 posts)as the baby boomers age.
I understand the want for job security but that doesn't seem to be a logical motivation for nurses endorsing Bernie, furthermore even "if" it were the case, they at least contribute to actual health care, the same can't be said for the private for profit "health" insurance corporations.
I also note that you poo poo the nurses in regards to supporting Bernie and his health plan for job security purposes and yet defend the much higher paid doctors from possibly having to take a salary cut.
There is no logical need to have for profit "health" insurance corporations and really what it all boils down to is what should societies value the most, greater health care for all its' people or just enjoy a few relatively well paid specialists.
Recursion
(56,582 posts)That's literally the entire point of this post: doctors and hospitals need to make a lot less than they do, and I think we need to be up-front about that. And, I don't think changing financing models is the way to make that happen.
Medicare for all could just ration health care in the same way the VA and military medical ration health care (long waits for appointments, time wasting bureaucracy, long lines in emergency waiting rooms).
Response to Recursion (Reply #22)
Uncle Joe This message was self-deleted by its author.

deathrind
(1,786 posts)A funded and fully staffed accounting department would a good place to start.
"Other Professional Services" $84 billion...
What is that?
I got an ambulance ride about a decade ago and the bill that followed was $800.
$300 for BLS
$500 for ALS
Turns out one stands for "Basic life Support" the other "Advanced Life Support"
The basic life support was the gauze bandage...the advanced life support was for the IV saline solution.
I have had great exposure to hospitals/care providers and insurance co over the last tens years between my mothers terminal illness and my grandmothers slow decline and passing at 88 this past year. Bandages $8, Tylenol $6, Bedpan $23, Chest X-Ray $1800, Misc service (as stated in the itemized bill) $2200. Most of the $ could come out just fair pricing. Another big chunk come come from getting rid of the part D that forbids price negotiations on pharmaceuticals. The last 16hrs of my grandmother life was spent in an ICU unit, the cost for that 16hrs...$85k...are kidding me. I was there for a good portion of that time. She got pain mgt, food and an IV...

question everything
(47,437 posts)for shuffling papers.
Recursion
(56,582 posts)closeupready
(29,503 posts)suddenly stops happening, and when it happens with the 65-year-old woman, it's closer to cost than the 50 bazillion dollars getting charged now.
Recursion
(56,582 posts)closeupready
(29,503 posts)it was just someone with health insurance, nobody checking the bills, bingo bango bongo, it got paid. Not sure how common it is, but I was just using that as an example of how there are hospitals which get away with some really scandalous monkey business.
Recursion
(56,582 posts)Hell, my old GP just got out of jail for it (that was an awkward call cancelling my appointment a few years ago...).
Single payer is financing reform. It doesn't change the incentives for providers.
closeupready
(29,503 posts)to provide a minimum level of health care for everyone, and costs come down - no more using emergency rooms for routine checkups.
Recursion
(56,582 posts)Medicaid's is $50 billion on $495 billion, or 10%
Private insurance's (including profit) is $122 billion on $991 billion, or 12%
From an overhead perspective, the best category of spending is out of pocket, which by definition has 0 overhead; if you want to eliminate overhead the government should just give people money with which they then purchase healthcare services (and that's actually not a horrible idea).
closeupready
(29,503 posts)It won't keep health care costs down either; as with student loans, unscrupulous parties will find ways to raise prices even further.
No, you need the bargaining power of Uncle Sam to control costs.
Recursion
(56,582 posts)Single payer does not change providers' incentives to do as much care as possible as expensively as possible. If anything it reinforces it, since attempts to cut their reimbursements can now be attacked as "cutting Medicare" and so become politically toxic.
closeupready
(29,503 posts)I'm not sure we do. I'm sorry, it's late, maybe I'm misreading your thread, I'll come back to it when I'm fresher. Thanks for the interesting discussion, by the way. 
closeupready
(29,503 posts)Recursion
(56,582 posts)From the same spreadsheet I linked, Table 4, "National Health Expenditures by Source of Funds and Type of Expenditures: Calendar Years 2008-2014"
Total gross spending (including overhead & profit):
Out of Pocket: $330
Private Insurance: $991
Medicare: $618
Medicaid: $495
Total non-overhead expenditures:
Out of Pocket: $330
Private Insurance: $869
Medicare: $580
Medicaid: $445
Medicare took in $618 Billion and paid out $580 Billion to providers. That's 6%. I'm not sure where the 2% myth came from (it's roughly 2% of total healthcare spending, which may be the source?) but these numbers are from Medicare itself. Medicaid, meanwhile, is at 10%, which is only barely less than private insurance.
applegrove
(118,497 posts)parking lots. There are some pretty fancy cars there. Those mostly belong to nurses and doctors. They do fine in Canada.
Recursion
(56,582 posts)Skwmom
(12,685 posts)do I want to list them for you? No, I'll pass.
On edit: This kind of stuff is one of the reasons this country is SUCH a mess.
Recursion
(56,582 posts)Which rows do you want to go down, and by how much? Broad-brush estimates are fine.

fwiff
(233 posts)In Canada, GPs make about 150k compared to 185k here. Specialists make more. Surgeons make most.
There has a been a freer market here, but that is changing with these big provider conglomerates. The medical industry is changing. Doctors are becoming employees these days, with lower earnings sucked up by the huge networks.
There are thousands of for profit hospitals, big group networks that skim doc's pay and supposedly not for profit orgs that are raking in HUGE profits.
Single payer will end up streamlining the process. How much time is taken up with insurance company shenanigans? How many billing hours? How much support staff?
Medicare reimbursement rates will have to be reworked.
Your guy O"M has some very good ideas on cost/service provisions.
At the moment it's a work in progress. Every other wealthy country has worked out a way. We spend more than double per capita of other countries-
Here's a good place to start
http://www.pbs.org/newshour/rundown/why-does-health-care-cost-so-much-in-america-ask-harvards-david-cutler/
Recursion
(56,582 posts)Last edited Thu Jan 28, 2016, 04:56 AM - Edit history (1)
The thought seems to be that too many Canadians (EDIT--I'm talking about Canadian doctors, not patients) cross the border because they make so much more, so they face at least a potential physician shortage.
There are thousands of for profit hospitals, big group networks that skim doc's pay and supposedly not for profit orgs that are raking in HUGE profits.
Yep. And hospitals on the whole need to make about half of what they do now, while serving 80 million more people.
Single payer will end up streamlining the process. How much time is taken up with insurance company shenanigans? How many billing hours? How much support staff?
All of which are part of those line items, and need to be drastically cut.
Your guy O"M has some very good ideas on cost/service provisions.
He definitely does, and I think it's the only realistic plan: use capitation and global budgeting to hold costs essentially where they are while the economy "grows to meet them", if that makes sense.
We spend more than double per capita of other countries
I know, and my point is it's mostly going to hospitals and doctors, not to insurance companies.

polly7
(20,582 posts)Recursion
(56,582 posts)polly7
(20,582 posts)Canadian doctors are not crossing the border for higher wages. That's an old, tired meme.
Recursion
(56,582 posts)polly7
(20,582 posts)Recursion
(56,582 posts)polly7
(20,582 posts)I said, that's a lie.
Our 'doctor shortage crisis' is, also.
Recursion
(56,582 posts)they listed in their most recent annual report
https://www.cihi.ca/en/nhex_2014_report_en.pdf
I still have no idea why you're trying to convince me Canada has a good health care system; I know that. I off-handedly mentioned one of the very few complaints people have (that lower physicians' salaries drive some physicians across the border).
If that's not what's doing it, I'd be curious to find out why Canada has fewer physicians, and particularly fewer specialists, per capita (Canada actually has more GPs per capita than the US, but fewer physicians as a whole).
polly7
(20,582 posts)across the border, because it's not true. In fact, more physicians from the U.S. are moving here because what they may lose in salary, they make up for by not having the huge overhead with insurers and staff to attend to all that entails, the increased insurance, threat of law-suits, etc. ... and the frustration many feel at having those without health-care knowledge at all telling them how and when they're allowed to provide diagnosis and treatment. I asked a young friend who's now a GP in a clinic and hospital near me if he would ever consider leaving for the U.S. to work, he looked at me like I had two heads (no offence).
Recursion
(56,582 posts)And just as a factual statement people -- even on DU, recently -- have complained about that. Are they wrong? Could well be. (And, for that matter, the complaint I've actually seen most is "this is why we have to get so many doctors from India and Bangladesh", and that's only been from people in BC, so the complaint is not about a current shortage but about the immigration policies being used to prevent one.)
polly7
(20,582 posts)out-dated memes about our system. Strange, that, when I never here those same things up here. We get doctors from all over the world, even the U.S. Should we complain about them? I don't think so, but maybe you should ask your Canadian friends.
Recursion
(56,582 posts)Good idea. Both are South Asian, so for all I know they're who my BC friend is griping about.
polly7
(20,582 posts)our system swirl down the drain. We have plenty of those - they love the idea of privatizing everything here.
Recursion
(56,582 posts)Which is it?
polly7
(20,582 posts)Last edited Thu Jan 28, 2016, 06:48 AM - Edit history (1)
you .......... you are the one saying it, I'm just telling you to ask them about my questions. Maybe you can get back to me on their replies, I don't know who they are to ask. Certainly, no-one I know has ever made those kind of RW nutjob statements.
I said "we have plenty of right wing nutjobs who would like to privatize everything."
Your spin must get dizzying.
polly7
(20,582 posts)Recursion
(56,582 posts)polly7
(20,582 posts)Last edited Sun Jan 31, 2016, 09:10 AM - Edit history (4)
https://www.cihi.ca/sites/default/files/document/nhex_trends_narrative_report_2015_en.pdfCheese Sandwich (4,130 posts) "Canada's Single-Payer Healthcare System Explained"
http://www.democraticunderground.com/1017301919
http://www.democraticunderground.com/10027521337
http://www.democraticunderground.com/10026727625 - "THIS is what Healthcare is all about ..."
I don't want to use NanceGreggs' tragic loss for anything detrimental, but feel her thread and what she and Jeff went through is exactly typical of all I've seen of our system, having worked in it for a long while, used it all my life and been an advocate for a huge family and friends who've gone through some very complicated and serious health issues. And again NanceGreggs, I'm very sorry for your loss.
Just a few more discussions with informative posts from a very quick search just here on DU debunking the 'horrific wait times and limited care' myths (proclaimed in the first link):
Ichingcarpenter (35,626 posts) "Canadian doctor schools U.S.Republican Senator on public health care"
http://www.democraticunderground.com/10024655743
http://www.democraticunderground.com/?com=view_post&forum=1002&pid=4658292
This video was both infuriating and interesting. Please do have a look at the 3:59 mark.
Re Premier Williams surgery in the U.S. Burr was gloating about:
17. The Peter Munk Cardiac Centre in Toronto, pioneers of the surgery he received:
PMCC FIRSTS IN CARDIOLOGY
For more than 75 years, we have been leading the way in innovative cardiac discoveries:
1935: First clinical use of heparin
1950: First pacemaker
1955: First successful valve transplant
1965: First coronary intensive care unit
1980: First prospective study of iliac angioplasty
1985: First mitral valve chordal replacement with expanded olytetrafluoroethylene
1986: First stentless aortic valve
1987: First aortic valve replacement using the Toronto Heart Valve
1988: First aortic valve-sparing operation
1990: First viral heart disease genetic test
1999: First sleep apnea clinical trial
2006: First discovery of the “SOS distress signal”
2009: First heart monitor recorder – CARTO 3 System
http://www.uhn.ca/PMCC
He also said he would inevitably have been seen as a queue-jumper if treated in Canada. But Dr. Jeanmart in Montreal said prompt care is available when the individual case is acute. The Peter Munk Cardiac Centre in Toronto said it has no extensive waiting list for any heart surgery at the moment.
"This is my heart, it's my health, it's my choice," Mr. Williams said. Of course it's his choice, but it reflects on the quality of medicare. The message he has sent by word and deed is that Canadian medicine is stuck in the past century.
http://www.theglobeandmail.com/globe-debate/editorials/a-choice-that-belittles-canada/article4388327/
More on that surgery:
http://www.theglobeandmail.com/life/health-and-fitness/williamss-heart-surgery-choice-was-based-on-ignorance/article1365308/
Please keep this in mind re watching Sally Pipes' testimony and who she is and what she stands for:
TrollBuster9090 (3,005 posts)
69. SALLY PIPES SHILL ALERT: (Just FYI)
Every time I see Sally Pipes spreading her anti-healthcare garbage I want to barf. But I'm not surprised the Republicans invited her. She's part of the wingnut welfare crowd.
Just FYI, there are two paid shills who Republicans usually invite to these dog and pony shows. One is Sally Pipes, who runs a paid, right-wing 'think tank' (aka Propaganda outlet) whose soul purpose is to put out propaganda trashing single payer healthcare systems with cherry picked data. No surprise she appeared here.
The other standard paid shill the Republicans usually invite is Dr. David Gratzer, who was trained as a psychiatrist in Canada, wrote a (self-published) book about how shitty the Canadian healthcare system is WHILE HE WAS STILL A MEDICAL STUDENT, and had no experience of it; and (like his commrade Charles Krauthammer) soon discovered that there was a lot more money to be made as a paid propagandists than there is as a doctor; and moved to NY to do that before ever having seen a single patient.
Gratzer is usually their token Canadian doctor that they always invite to trash the Canadian healthcare system. I don't understand why they didn't invite him! They must be slipping.
I can only conclude that Gratzer is affraid to show up at any hearing where Sanders is present, because the last time he was invited to a hearing with progressives present, Dennis Kuchinich ripped him a new asshole.
Watch this video of Kuchinich taking the little turd apart. It'll make your day. http://www.democraticunderground.com/?com=view_post&forum=1002&pid=4660362
http://www.dailykos.com/story/2008/4/5/488434/- Sally Pipes is an unethical hack
Top Obamacare Critic's Op-Eds Drafted by PR Firm That Reps Drug, Health Care Clients - Meet the magic PR elves fueling Sally Pipes' pro
http://www.motherjones.com/politics/2012/07/sally-pipes-pacific-research-institute-keybridge-communications
eridani (48,829 posts) "Why do Canadians so strongly support their single payer system?"
http://www.democraticunderground.com/10026223948

National Health Expenditure Trends, 1975 to 2015:
https://www.cihi.ca/sites/default/files/document/nhex_trends_narrative_report_2015_en.pdf
https://secure.cihi.ca/free_products/trends_in_income_related_inequalities_in_canada_2015_en.pdf
So really ...... those who are trying so hard to make it appear what it isn't, will just have to try a bit harder - there are actually people on here who know the truth of what we get and wouldn't trade it for anything. Period.
8 facts that explain what’s wrong with American health care
Updated by Sarah Kliff on January 20, 2015, 9:58 a.m. ET
If the health-care system were to break off from the United States and become its own economy, it would be the fifth-largest in the world. "It would be bigger than the United Kingdom or France and only behind the United States, China, Japan, and Germany," says David Blumenthal, executive director of the nonprofit Commonwealth Fund.
Or here's another way to put it in its (ridiculous) perspective: The US, which has a mostly private health-care system, manages to spend more on its public health-care system than countries where the health-care system is almost entirely public. America's government spends more, as a percentage of the economy, on public health care than Canada, the United Kingdom, Japan, or Australia. It spends even more than that on private health care.
Americans are not equal health-care spenders. There are a handful of patients who use lots of medical services — and tens of millions of people who barely go to the doctor at all.
http://www.vox.com/2014/9/2/6089693/health-care-facts-whats-wrong-american-insurance
Canada's health plan doesn't cover certain services. Non-cosmetic dental care is covered for children up to age 14 in some provinces. Outpatient prescription drugs are not required to be covered, but some provinces have drug cost programs that cover most drug costs for certain populations. In every province, seniors receiving the Guaranteed Income Supplement have significant additional coverage; some provinces expand forms of drug coverage to all seniors, low-income families, those on social assistance, or those with certain medical conditions. Some provinces cover all drug prescriptions over a certain portion of a family's income.
Private Health Insurance
While the health care system in Canada covers basic services, including primary care physicians and hospitals, there are many services that are not covered. These include things like dental services, optometrists, and prescription medications.
Private health insurance plans are usually offered as part of employee benefit packages in many companies. Incentives usually include vision and dental care. Alternatively, Canadians can purchase insurance packages from private insurance providers.
The main reason many choose to purchase private insurance is to supplement primary health coverage. For those requiring services that may not be covered under provincial health insurance such as corrective lenses, medications, or home care, a private insurance plan offsets such medical expenses.
While private insurance can benefit those with certain needs, many Canadians choose to rely exclusively on the public health system.
http://www.canadian-healthcare.org/page4.html
We've always had private/third party insurance plans that, depending on the province and what the consumer chooses, covers what our health-plan may not (keeping in mind the above services already expanded for low-income families and individuals and children as well as seniors), including: certain out-pt. prescription drugs/medicines, semi-private or private hospital accommodation (though I've seen many/most times those without any insurance placed in semi-private or private rooms - most in my family even without insurance have always been placed in semi-private rooms, if not private - especially in the smaller hospitals), special nursing services, regular ambulance services, artificial limbs, prostheses and medical appliances, wheel chairs and other durable equipment, specified medical or paramedical services that fall outside government plans (ie., chiropractors, physiotherapists, podiatrists, osteopaths and optometrists) and vision care (eyeglasses and contact lenses). Dental services are often covered under a separate supplementary insurance plan.
And, more ..... disability insurance, critical illness plans, living benefits, long-term care insurance, additional travel insurance, etc.
Many of the above additional expenses are reimbursed or partially reimbursed through allowable personal income-tax deductions.
http://www.democraticunderground.com/?com=view_post&forum=1251&pid=1030919
http://www.taxtips.ca/filing/medicalexpensetaxcredit.htm
It works for us, and every day each province/territory is looking for ways to improve it.
Canada Health Act:
The Canada Health Act (CHA or the Act) is Canada's federal legislation for publicly funded health care insurance.
The Act sets out the primary objective of Canadian health care policy, which is "to protect, promote and restore the physical and mental well-being of residents of Canada and to facilitate reasonable access to health services without financial or other barriers."
The CHA establishes criteria and conditions related to insured health services and extended health care services that the provinces and territories must fulfill to receive the full federal cash contribution under the Canada Health Transfer (CHT).
The aim of the CHA is to ensure that all eligible residents of Canada have reasonable access to insured health services on a prepaid basis, without direct charges at the point of service for such services.
The Canada Health Act is federal legislation that puts in place conditions by which individual provinces and territories in Canada may receive funding for health care services.
http://www.hc-sc.gc.ca/hcs-sss/medi-assur/cha-lcs/index-eng.php
There are five main principles in the Canada Health Act:
Public Administration: All administration of provincial health insurance must be carried out by a public authority on a non-profit basis. They also must be accountable to the province or territory, and their records and accounts are subject to audits.
Comprehensiveness: All necessary health services, including hospitals, physicians and surgical dentists, must be insured.
Universality: All insured residents are entitled to the same level of health care.
Portability: A resident that moves to a different province or territory is still entitled to coverage from their home province during a minimum waiting period. This also applies to residents which leave the country.
Accessibility: All insured persons have reasonable access to health care facilities. In addition, all physicians, hospitals, etc, must be provided reasonable compensation for the services they provide.
http://www.canadian-healthcare.org/page2.html
Federal transfers are allocated to each province to manage and deliver health services.
Canada's national health insurance program, often referred to as "Medicare", is designed to ensure that all residents have reasonable access to medically necessary hospital and physician services, on a prepaid basis. Instead of having a single national plan, we have a national program that is composed of 13 interlocking provincial and territorial health insurance plans, all of which share certain common features and basic standards of coverage. Framed by the Canada Health Act, the principles governing our health care system are symbols of the underlying Canadian values of equity and solidarity.
Roles and responsibilities for Canada's health care system are shared between the federal and provincial-territorial governments. Under the Canada Health Act (CHA), our federal health insurance legislation, criteria and conditions are specified that must be satisfied by the provincial and territorial health care insurance plans in order for them to qualify for their full share of the federal cash contribution, available under the Canada Health Transfer (CHT). Provincial and territorial governments are responsible for the management, organization and delivery of health services for their residents.
http://www.hc-sc.gc.ca/hcs-sss/medi-assur/index-eng.php
Making Medicare - The History Of Health Care In Canada 1914-2007
http://www.historymuseum.ca/cmc/exhibitions/hist/medicare/medic00e.shtml
The poor who cannot afford dental, ect. not paid for by the health care program can get help:
Here's a quick look at who is eligible for what:
http://www.fptdwg.ca/English/e-access.html
http://www.caphd.ca/programs-and-resources/government-dental-programs
http://www.health.gov.sk.ca/supplementary-health-program
.............................
In some provinces any child under 14 is eligible under the Canada Health Act for full dental coverage that is not cosmetic.
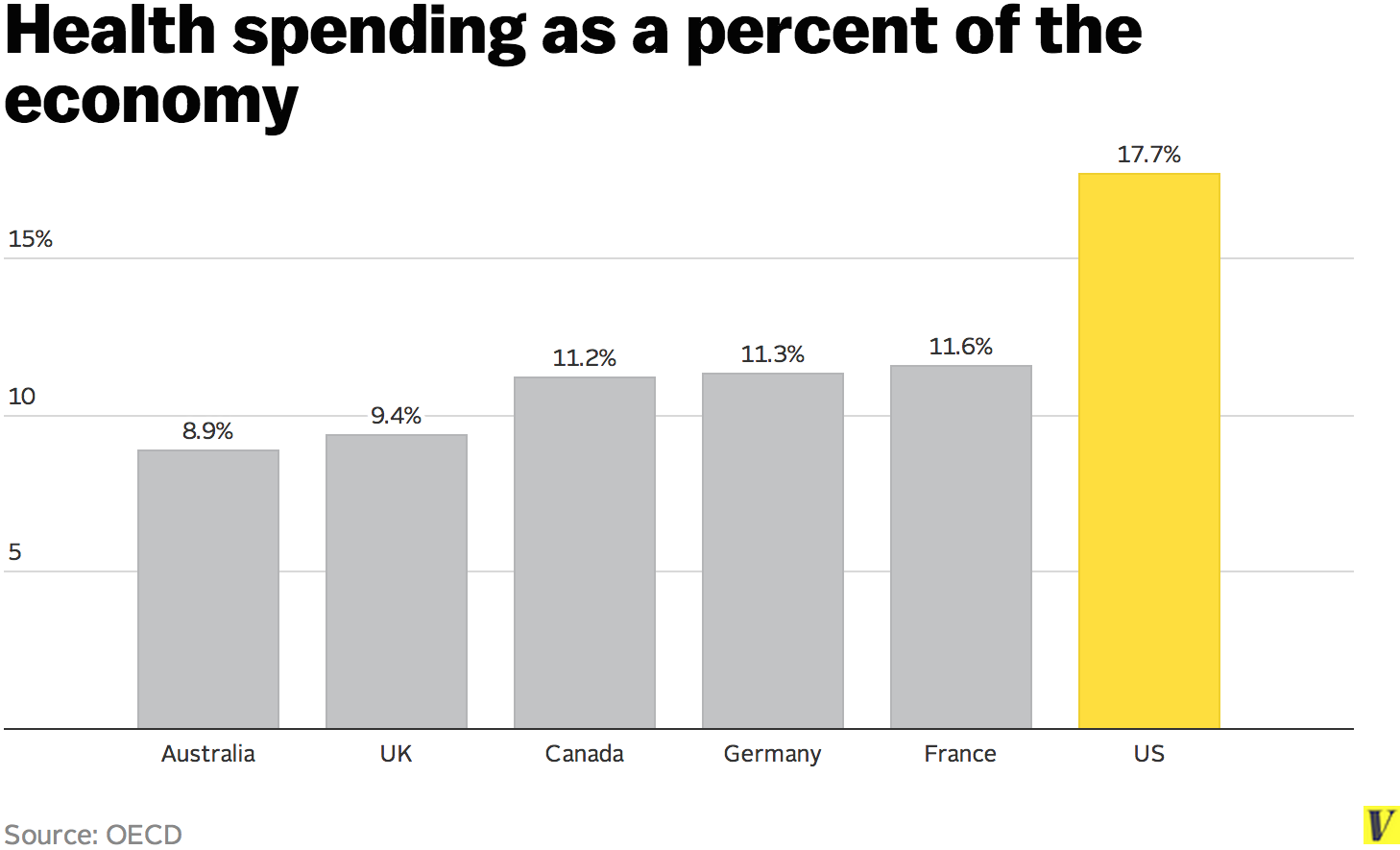
Canada spends 11.2% on health care versus 17.7% in the U.S.- with better outcomes in both infant mortality rate and life expectancy. I don't know much at all about your taxes, but I would rather pay mine knowing that most of it goes to ensuring quality health-care for all, than paying to mainly support the MIC while watching millions of people die without access to health services other than the E.R.
http://www.vox.com/2014/9/2/6089693/health-care-facts-whats-wrong-american-insurance
Btw ......... how about your wait times and quality of care, does everyone there get diagnostics and specialist appt's, treatments as promptly and with the high quality as we do? I hope so! I've never had to wait more than three days to see a doctor anywhere I've lived. Here it's usually that afternoon or the next day and if it's something serious the doctor quite often calls the specialist while I'm sitting there and books an app't., usually within days or weeks ... depending upon the illness. If I've heard something about a specialist I'd rather see ....... I'm perfectly free to ask for her/him.
I have never had to pay one single penny out of pocket nor has anyone else unless they've wanted a private room (which very few people I know even care about - the rooms in our smaller hospitals are all private anyway). We keep our gas and hotel receipts for driving, parking and staying in the city to claim back at income tax time. I've worked in health-care in different positions much of my life and been an advocate for members of a huge family and group of friends for many more, and have never seen otherwise, except for cataract surgery and hip replacements for older family members --- those did have wait times.
What about elective and non-emergent issues - is everyone there assured of the same high-quality treatment and care even if they have to wait for it? I hope so!
Absolutely, our system is far from perfect ....... but we are always working on ways to improve it. Committees made up of physicians, nurses, First Nations representatives, social service representatives, etc, - province by province and territory. It is an ongoing process and always will be.
Final comment from the first video: "Those in the United States who are concerned about health-care spending and what it means to the economy might respect that course of action. But instead, we attack. That's our problem, not theirs."
I'll just keep reposting this whenever you trot out yet another of your hit-threads.
Recursion
(56,582 posts)Since I agree it's pretty good, I'm not sure why you posted it here.
polly7
(20,582 posts)polly7
(20,582 posts)Sure. 
Look, if it makes you feel better to think that I am making up having friends north of the 48th parallel, and that they think this, go for it.
(For the record, from what I have seen they're wrong, at least on a national level; to the extent there are shortages they seem to be regional.)
polly7
(20,582 posts)Do you have an excess of clinics and medical workers in remote areas? How about on Native reservations - are there a lot of doctors and specialists available right there?
Most of our doctor shortages occur in remote areas, we're continuously working at providing better health-care accessibility to places that ARE lacking it, and freely admit there needs to be much more work to be done.
Do your health-care providers/insurers provide 1st quality health-care in places like Pine Ridge - or any severely depressed economic area for those who can't afford to spend a single dime to get care?
polly7
(20,582 posts)Recursion
(56,582 posts)I don't think simply adopting its financing model wholecloth will help the US much, because Canada's financing system is only a small part of what makes it work so well.
polly7
(20,582 posts)They get tiresome in every identical thread you state them on.
Recursion
(56,582 posts)Do you have an excess of clinics and medical workers in remote areas? How about on Native reservations - are there a lot of doctors and specialists available right there?
Are you somehow under the impression that I think the US's healthcare system is better than Canada's, or even "good" in any absolute sense on its own? I don't.
polly7
(20,582 posts)Answer MY questions.
I've responded to your 'anecdotes'.
Recursion
(56,582 posts)The US has serious local physician shortages in multiple communities, particularly rural ones, and particularly majority Native American and African American areas. There is a similar but not quite as bad shortage in poorer urban areas. Meanwhile there's something of a glut in rich exurban areas. Doctors seem to congregate where the money is. The FQHC system is an attempt to fix that but it needs to be much, much bigger (and O'Malley wants to expand it significantly).
Interestingly, both the US and Canada have
1. Fewer physicians per capita than the OECD average, and
2. Higher physician pay per capita than the OECD average
Canada manages to make that work. We don't.
polly7
(20,582 posts)I guess we're not all that different, but I'd bet every cent I own we are doing a much better job of working every day of every month to address our problems. Are your insurers doing the same?
Recursion
(56,582 posts)No, they're not. Nor are our doctors, our drug manufacturers, our hospitals, our nurses, our dentists, our device manufacturers, our lawyers, or our politicians. All of those are more or less doing the right thing in Canada (OK, probably not the lawyers), and all of them more or less aren't here.
polly7
(20,582 posts)every few days. I'm not confused with your goal whatsoever.
Recursion
(56,582 posts)I haven't talked about the alleged Canadian doctor shortage before, though other people on threads I've started have.
polly7
(20,582 posts)Recursion
(56,582 posts)I really have no idea who or what you think you're attacking, but this is getting silly.
Here are the inputs to Canada's system compared to the US's:

And here are the outputs:

You guys are doing this much better. But I don't think your financing (the "overhead" bar in the expenses) is the reason. I think the your hospitals' and doctors' business models and charters are the reason, and I think the bars in that second chart bear me out. We pay hospitals and doctors a lot more than you do.
polly7
(20,582 posts)You using your 'Canadian friends doing all that grumbling' - even so far as bigotry against physicians from other countries you're spreading here, as on this thread, are the attacks ..... wouldn't you say?
Recursion
(56,582 posts)And, no, I wouldn't say I've attacked it at all. I've been consistently praising Canada's system.
closeupready
(29,503 posts)Something must be done. I don't know what, but Bernie is the only one who is talking about doing something about it, and I think we'd all survive. As things are, many people do NOT survive.
Recursion
(56,582 posts)Maryland was the only state to see hospital costs go down over the past decade, after they adopted global budgeting (a.k.a. "all payer" if you need something that works on a bumper sticker).
closeupready
(29,503 posts)it's insufficient. K&R

mhatrw
(10,786 posts)Rosa Luxemburg
(28,627 posts)Healthcare should not be a business
mhatrw
(10,786 posts)worth a several dollars of ICU and emergency room cure!
It's not rocket science. Stop all corporate and individual profiteering on healthcare, emphasize relatively inexpensive PREVENTATIVE care, and 99% of us will save a bundle.
Recursion
(56,582 posts)Sanders wants to change the financing methods we use on healthcare while leaving the for-profit provider system intact.
O'Malley wants to directly limit the budgets of hospitals (the big cost center here; see above) based on the populations they serve so that hospitals have to charge less for the procedures they perform.
mhatrw
(10,786 posts)their "richly deserved" slice of the pie!

uponit7771
(90,304 posts)
FSogol
(45,448 posts)
brewens
(13,539 posts)Recursion
(56,582 posts)Sanders wants to reduce healthcare spending by $1.7 Trillion.
Absolutely eliminating all private insurance overhead saves nearly $200 billion.
Which rows do the other $1.5 Trillion come from?
brewens
(13,539 posts)the best deal, not the worst.
Recursion
(56,582 posts)So, we've got magically over-head free financing, and magically free pharmaceuticals.
You still need to find $1.2 Trillion from the remaining rows.
While allowing the 80 million people (25% of the country) currently skipping treatments for cost to have access to those treatments.

Nye Bevan
(25,406 posts)Unthinkable!
Last August, Baer Hanusz-Rajkowski, of Bayonne, accidentally cut his finger with the claw-end of a hammer. He says he waited a few days for it to heal but the cut didn’t seem to be closing, so he went to the Bayonne Medical Center emergency room to ask whether he should get stitches. The nurse practitioner determined no stitches were necessary, he says. There was no X-ray either.
Instead, Hanusz-Rajkowsk got hit with an $8,200 bill for the emergency room visit. On top of that, Bayonne Medical Center charged $180 for a tetanus shot, $242 for sterile supplies, and $8 for some antibacterial ointment in addition to hundreds of dollars for the services of the nurse practitioner.
“I got a Band-Aid and a tetanus shot. How could it be $9,000? This is crazy,” Hanusz-Rajkowski said. “If I severed a limb, I’d carry it to the next emergency room in the next city before I go back to this place."
http://www.nbcnewyork.com/news/local/I-Team-NJ-Hospital-Charges-8K-to-Bandage-a-Cut-Finger-270053241.html
Recursion
(56,582 posts)Which, again, gets to the point that financing reform doesn't actually fix these problems.
Nye Bevan
(25,406 posts)but I thought Medicare had detailed fixed price schedules for every possible procedure and test?
Recursion
(56,582 posts)1. All of those prices are too high, including Medicare's, and
2. Those price schedules give hospitals the incentive to perform the most expensive treatment possible.
This is why O'Malley wants to move to paying by outcomes, not by inputs.
Skwmom
(12,685 posts)Recursion
(56,582 posts)AgingAmerican
(12,958 posts)From the Obamacare debate
Recursion
(56,582 posts)I don't see how you can possibly complain about that question
AgingAmerican
(12,958 posts)From the Obamacare debate
Recursion
(56,582 posts)OK, then.
AgingAmerican
(12,958 posts)Of course I do.
But that doesn't matter, because this OP is pushing a GOP talking point from the Obamacare debate.
Recursion
(56,582 posts)Where does the other $1.5 Trillion come from? Which of those rows do you want decreased?
AgingAmerican
(12,958 posts)Not $200 billion once.
http://healthcareforamericanow.org/ourissues/health-insurance-industry/
And how many years is that $1.5 trillion number over?

Recursion
(56,582 posts)Private insurance overhead (including profit) which I posted in the OP from Medicare's own numbers is $195 billion off of $991 billion in premiums paid in 2014.
So, it's currently a $991 billion dollar industry, of which $195 billion is overhead and profit.
AgingAmerican
(12,958 posts)Single payer is cheaper with better outcomes.
Recursion
(56,582 posts)But it's definitely not cheaper unless we find a way to claw back reimbursement rates very far.

CajunBlazer
(5,648 posts)The devil is always in the details. It's interesting to see how people who have totally bought into a plan get all confused when they have to figure out how it could possibly work.
+ a gillion
closeupready
(29,503 posts)and other similar Western countries with a national health insurance program?
I think when you look at differentials in cost, you'd quickly find a large portion (perhaps all) of that $1.5T in the fact that Americans with health insurance are being overcharged for EVERYTHING.
When a private business wants to cut costs, they don't do a line-item type examination and account for every cent (though perhaps they should); no, what they do is go to middle managers and tell them, "I don't care where you cut, but I want you to get costs to such-and-such a level". And mostly, it gets done. Likewise, Medicare could say the law mandates basic coverage; they send in auditors and demand aspirin comes down from like $50 per pill to 50 cents, you know, that kind of thing.
As others have said, I'm no expert, I just don't see why you feel a need to see everything with such specificity.
Recursion
(56,582 posts)The differences are kind of telling, to me:
(This is from the 2013 version of the CMS report, and the analogous Canadian report. In the bar graphs, all costs are 2013 US dollars, and Canada is on the left with the US on the right.)




closeupready
(29,503 posts)That is, officials whose job it is to examine costs to make sure the government isn't being overcharged?
Recursion
(56,582 posts)Also, just as grist for the mill, Canada has 2.2 doctors per 1000 people while the US has 2.4 doctors per 1000 people; however, Canada has about 1.2 GPs per 1000 people and 1.0 specialists, while the US 0.6 GPs per 1000 people and 1.8 specialists. That's got to mean something...
SheilaT
(23,156 posts)It's over 50k per year, most of which winds up being borrowed money. I strongly suspect that doctors in other countries do not start their professional lives under a mountain of debt.
Among the reforms I'd like to see is that medical school costs be greatly reduced. If not made free, no more than 10k per year, which is a manageable amount. If doctors could start their careers with little or no debt, I suspect many more of them would go into primary care, or gerontology, two areas where more doctors are needed, but aren't very highly paid. Our current system strongly encourages doctors to look at what specialties pay the most, rather than where they'd most prefer to practice.
Also, a true Universal Health Care system, where everyone's health care needs were actually met, would vastly reduce lawsuits, which would benefit pretty much everyone.
Recursion
(56,582 posts)They don't. But single payer doesn't impact medical school costs.
Also, a true Universal Health Care system, where everyone's health care needs were actually met, would vastly reduce lawsuits, which would benefit pretty much everyone.
I believe tort reform has a role to play, but I don't think it's as big as a lot of people claim. I don't have any numbers with me right now to back that up, but I'll see what I can dig up.
SheilaT
(23,156 posts)but most other first world countries offer secondary education at a fraction of what we charge our students, even at public colleges and universities. I likewise suspect their med students don't pay a lot of money for their medical school. It comes down to what a culture considers important.
In this country, it's guns and the military. We will pay anything at all to maintain a world wide military presence, to invade or bomb other countries at will. We also find it acceptable that thousands of people die from gun violence every year. Other countries have vastly smaller military, vastly fewer guns. Not only do far fewer of their citizens die from war or guns, but they have money left over to pay for school and medical care. How odd is that?
Recursion
(56,582 posts)They do, and we should (I'll also take this opportunity to plug O'Malley's debt free college proposal: https://martinomalley.com/policy/make-college-debt-free/ which much like is healthcare plan is addressed more at the actual providers than at the financing questions).
OTOH many of those countries also much more strictly limit who can go to college to begin with (though they have excellent technical and trade schools and apprenticeship programs instead, which, again, is a good thing).
Not only do far fewer of their citizens die from war or guns, but they have money left over to pay for school and medical care.
Very good point.
SheilaT
(23,156 posts)which I see as a mixed blessing. On one hand, I like living in a country where anyone can go to college. On the other, there are a lot of people who have no business going to college, and there are lots and lots of ways to earn a good living that doesn't involve four years of college.
Our community colleges tend to have excellent degree programs that lead to good jobs, and many more people should go that route. Alas, the notion that *everyone* is entitled to four years of college has taken hold, and it's hard to get people to understand exactly what's wrong with that.
Plus, of course, it's possible to go on with your education later. I did once get into a disagreement with someone here on DU who felt completely justified in taking some academic program that was absolutely not going to lead to a good job (something along the lines of 17th Century French literature) but felt he could only do this now, at this point in his life, because once he had a job he could not possibly imagine putting forth the intellectual effort for whatever rather esoteric field of study he was in. He didn't even begin to consider how he was going to earn a living once he'd gotten his degree, and he could not even begin to entertain the notion of going to college for the sheer joy of the intellectual pursuit.
I'm someone who has attended college on and off almost all of my adult life, and I won't tell you how old I am, but I will mention that a few months ago I went to my 50th high school reunion. Going to school as an older adult has been a joy. I was able to work and take classes and it was wonderful. That's just me.
Hoyt
(54,770 posts)inner city area and you don't even have to pay it back. Not a bad return on investment.

Matariki
(18,775 posts)There would be a lot more doctors and their salaries wouldn't have to go toward hundreds of thousands of dollars in school debt.
Recursion
(56,582 posts)And in particular he wants to give tuition assistance to med students who then go work in public clinics in underserved areas.
artislife
(9,497 posts)Christ on a stick, how is this OP not RW bs?
Recursion
(56,582 posts)Can you cut the "right wing" crap here?
artislife
(9,497 posts)Poor doctors won't get as much re-imbursement.
That's true. Though they will still need staff to send claims, they won't spend time fighting with the insurers to get paid.
I worked in the billing offices of chiropractors. The insurance industry is the reason that there is a pay per fee problem. I spent half the time chasing insurance companies for the odd visit here or there, that somehow they didn't process. They made the portals to get information from a straight forward process to a maze of portals and different pages where it wasn't easy to see history.
I had some insurance companies that I had to send a fax to request benefits or claims status. FAX!!
They are almost as bad as Big Pharma.
So this little exercise of your OP gets me steamed. People in this country die because of the greed and bs that surrounds this subject. This is not some practice in theory, this is real.
And so to me, those who plant these seeds are not doing any real good for the side of liberalism.
Recursion
(56,582 posts)You're focused on single payer, one particular type of finance reform, to the detriment of universal affordable healthcare, which is the actual goal.
artislife
(9,497 posts)There is a meme going around that will help you understand my point of view..
A man sits with his head in his hands.
Before Obamacare he couldn't afford health insurance
After Obamacare he still can't afford health insurance, but the IRS is fining him for being unable to afford it.
You say affordable, so did Obama. Unfortunately, as it stands it is the Insurance companies that define what affordable is.
uponit7771
(90,304 posts)uponit7771
(90,304 posts)... government seeing that high premiums is the real issue.
Going from 550 to 490 a month doesn't make me want to jump ship to Sanders
artislife
(9,497 posts)not only is the premium lower, but there would not be the whole in /out of network head ache. I went to the emergency room this holiday with a newly discovered shellfish reaction. After they treated me, they gave me a referral to an allergist. I couldn't go to him because he didn't take my insurance. The staff said the visit could cost a lot because they would run lab tests to see what else I could be allergic to.
It was days before the end of the year. I spent an hour on hold trying to reach someone to get the name of someone who could see me. I finally gave up. I carry epi pens now and am fearful of eating at most restaurants.
That isn't the bad part, there are posters here who had to pay for medical staff that came into surgeries that they had prequalified. Well, one of the team was Out of network and they had ghastly bills. This is the craziness. It is more than mere deductibles.
uponit7771
(90,304 posts)... along with lower bills.
A family of four shouldn't be paying more than 200 a month for HCI for the best plan
artislife
(9,497 posts)I think we have reached an agreement on an issue and I raise a glass to it!

Kentonio
(4,377 posts)Then the lower wage is more than acceptable. Of course its much more difficult in the short term, you can reduce existing debts, but for people who have already paid off their student debts it will probably seem totally unfair to suddenly take a big wage hit.
Big picture though I think it has to happen to move the system to where it needs to be. It's also worth mentioning though that universal healthcare does not mean the end to private insurance. The UK still has private healthcare for people who want it, which means there are still places where doctors are free to earn higher wages if they choose.
Recursion
(56,582 posts)Dr John Dean, a consultant cardiologist in Exeter, says NHS doctors who supplement their income by seeing patients privately end up compromising their ethics because they have a financial incentive to recommend treatment that may not be necessary.
Private healthcare deprives the NHS of doctors, increases waiting lists for care and does not give patients the superior treatment they think they are paying for, he argues.
“I have always been ambivalent about private practice, and I had become increasingly uncomfortable about my own involvement. I realised that, in all conscience, I could not go on with it,” Dean writes in an opinion piece in Wednesday’s edition of the BMJ, formerly the British Medical Journal.
slipslidingaway
(21,210 posts)you cannot. Stop posting news stories and tell us what system you want. A more socialized system where you pay your dues for a certain number years to the NHS or a system where you do not?
On one hand you praise what O'Malley is doing and then you you turn around and post a disparaging story about the system he wants? Should the docs participate in the NHS system or not, sorry I am really confused.
And do not even get me started on outcomes, yes that can help to a certain extent, but has that been tried in an inner city where they are sent home and told to take meds that they cannot afford, let alone have a support system at home? Penalizing the inner city hospitals is wrong. This is like penalizing a child who comes to school and has not had breakfast and now the inner city hospitals will get less money?
My sister has an excellent primary physician, either Oxford or Cambridge trained, not to quibble between Yale or Harvard, remember their student loans do not even come close to what they are in the US.
Do you see the docs in the US that have now INVESTED in their own private surgical suites?
My daughters future compensation is based not only on the number of patients she sees but also on COLLECTIONS! This is our damned for profit system! We need to realize the implications for the people of our country, my jaw dropped when salary was not only tied to the numbers of patients but also collections. You know how many in her graduating class were going into private practice, three, and two of those were joining an established family member's practice. All of the 70 plus, including my daughter, were joining a large for profit HC system. They saw the the opportunities, insurance nightmares. In essence enjoy shopping for all your HC needs or hardware needs at HD or Lowes, the concentration in HC is coming.
Sorry but you better realize what is taking place in our country before posting about other countries.
polly7
(20,582 posts)Recursion
(56,582 posts)This is absolutely ridiculous. I've had nothing but praise for Canada's, France's, Germany's, the UK's, and the Netherlands' health care system. Ours sucks. It absolutely sucks. Everybody else's is better. Financing is only a tiny part of that.
polly7
(20,582 posts)continuously, even after you've been proven wrong?
Sorry, I don't believe you one single, tiny bit.
Recursion
(56,582 posts)And even qualified that with "some people say". Which is in fact true: some Canadians (at least in your news media) have said that. And then went on to point out that Canada manages to provide more GPs per capita than the US does.
It was an off-handed way to introduce that Canada is still managing that better than we are.
Seriously, this is just silly.
polly7
(20,582 posts)Recursion
(56,582 posts)Huh? O'Malley isn't advocating single payer, he's advocating capitation-based global budgeting for hospitals and doctors (which is closest to France's system, and one I agree with), though his initial plan doesn't subsidize as much of the costs as France does or as much as I would like. I still think it's the only realistic way forward.
This is like penalizing a child who comes to school and has not had breakfast and now the inner city hospitals will get less money?
That is a downside. Maryland, at least, alters the targets based on the health and other problems in the area the provider serves.
Kentonio
(4,377 posts)Not just doctors who only work within the private sector. Not that very many people use private healthcare in the UK anyway, its mostly just richer folks wanting private rooms and added perks.
Recursion
(56,582 posts)Agreed.
If we adopted single payer, and didn't make it mandatory like Canada did, I wonder how many providers and patients in the US would prefer a private system?
Cheese Sandwich
(9,086 posts)polly7
(20,582 posts)Recursion
(56,582 posts)Single payer doesn't fix that.
Cheese Sandwich
(9,086 posts)Single payer won't fix that. OK. That's not a reason to oppose single payer. It's not a magic bullet that solves everything. It solves some things.
None of the candidates have a plan to ban for-profit hospitals. I don't see how the question of for profit hospitals is even relevant to the primaries since no candidates have raised the issue.
Recursion
(56,582 posts)Which, while not as good as ending them, directly limits the damage they can do.
It's not a magic bullet that solves everything. It solves some things.
With our provider structure it makes things worse. Once we have SP, every single attempt to push down hospital charges gets attacked as "cuts to Medicare".
Cheese Sandwich
(9,086 posts)Sounds like you're trying to convince me I won't be better off with a single national health insurance program. I'm not buying that, at all. I think Medicare will be able to set its own prices because it's the payer. They already set their own reimbursement rates. They don't have to pay what providers request.
Recursion
(56,582 posts)When Medicare funding falls short, Congress is left with two options: Cut doctors’ pay or appropriate additional funds. Legislators don’t really like the first one; they worry providers would flee the program if their salaries were slashed. So since 2003, under both Democratic and Republican control, Congress has passed short-term doc-fixes to keep provider payments stable (or, in some cases, give doctors a slight raise). These pay-patches have ranged from a few years to just 30 days. In 2010 alone, Congress has passed five separate doc-fixes, none longer than six months. Last December, Congress passed a one-year doc-fix that cost $19 billion and lasts til the end of 2011.
Incidentally, since that FAQ was written the "fix" (it would be better described as a "break", IMO) has been made permanent.
The worry about providers fleeing the program is why I keep asking, and keep not getting an answer to, this question:
Under Sanders's plan will billing outside of the Medicare For All system be legal?
Cheese Sandwich
(9,086 posts)They "overpay" because they fear doctors will flee the program if their pay is cut. That's why we should put an end to private health insurance and have one national health insurance program. Then if doctors want to flee the system they will have to move to another country where they can get paid more, which is nowhere good.
Recursion
(56,582 posts)That's two separate questions, isn't it?
We can establish a national health insurance system that everyone pays into and everyone can use. Canada and the UK did that (well, the UK directly pays the doctors, but the result is largely the same).
Separately, we can require that all payments for all covered medical procedures be done only through that financing system. Canada did that; the UK didn't.
Which one of those Sanders wants to adopt makes a huge difference in the kind of outcome it would have. I'm much more supportive of the mandatory system than the non-mandatory one, but that means making it actually against the law (as in, you'll go to jail) to be a doctor in private practice accepting private payments. I support that, but I think the public would be a lot more leery.
At any rate, I think it's absolutely absurd that Sanders released his "plan" without addressing that question.
Cheese Sandwich
(9,086 posts)Everybody, all the people of the US, will be on The Plan. It's going to be fucking awesome 
With everybody on The Plan doctors will have to accept The Plan or they won't have any patients.
Uphold the people's health plan.
Recursion
(56,582 posts)Oh, if it's legal, they'll have patients. Plenty of people won't want to be in a waiting room with hoi polloi, and will be willing to pay for that.
Cheese Sandwich
(9,086 posts)Being forced to mingle with the "hoi polloi" is a non-issue. Things really aren't going to change much at all except instead paying a private insurance company, we'll pay The Plan, and it will be way cheaper and have better outcomes. People will just go to the doctor and the doctor will accept the insurance. That's it. It's really that simple.
Recursion
(56,582 posts)Will doctors be legally allowed to bill privately for procedures that are covered by Medicare? (For instance, this is a criminal act in Canada.)
If they are, doctors will, and people will go to them. And a private insurance market will spring up to finance it.
polly7
(20,582 posts)Ownership usually resides with community-based not-for-profit corporations, religious organizations, or with municipal governments (as are ours in the more rural areas) or universities. Apart from psychiatric hospitals, provincial/territorial governments rarely own hospitals. In all cases, however, the vast majority of hospital revenues come from a single funder – the provincial/territorial department of health.
This includes all hospitals approved by provincial governments providing acute care, extended and chronic care, rehabilitation and convalescent care, and psychiatric care, as well as nursing stations and outpost hospitals.
Recursion
(56,582 posts)Adopting that model would be much more effective than simply copying Canada's financing system.
polly7
(20,582 posts)Recursion
(56,582 posts)And the fact that they're nearly all not-for-profit is a much bigger part of why you guys pay less than we do, than the fact that the financing is done through the government.
Canada's on the left, the US is on the right.
The amount we pay hospitals and doctors is the problem. The amount we pay in overhead is an annoyance.
Enrique
(27,461 posts)the people that want to move to single payer think that providing care should be the goal.
Recursion
(56,582 posts)If you absolutely eliminated private insurance overhead and profit, public insurance overhead, and pharmaceutical costs, you would need to find about $1 Trillion in the remaining line items to get health care spending that low.
Which ones do you think should be lowered, and by how much?
Enrique
(27,461 posts)my belief that single-payer is feasible is based on knowing that in many other countries it works, not because I have run the numbers.
Recursion
(56,582 posts)Literally every other country does something else to achieve universal health care

DanTex
(20,709 posts)I wish more people would understand that, in the dream world where the government administers the program at zero cost, single payer alone would save only $195B. Of course, in reality the savings are much less than that, because the government also has administrative costs.
All the rest of the savings are not related to the payment system, and can be achieved without SP. Will it be difficult? Sure. And it will also be difficult with SP. You can have government set prices. You can have all-payer rate setting. Etc.
But getting prices down means getting the cost of actual care down. Not the cost of insurance and overhead. It's going to difficult, and it's going to be disruptive, and hospitals are going to close, and all that, and whether it's single payer or not is really a side issue.
uponit7771
(90,304 posts)Sancho
(9,067 posts)The GOP and other Democrats will both point out the problem with paying health care workers much less. Most Democrats don't want anyone's salaries to go down or their taxes to go up! That's true of all the hard-working American heath care providers.
https://www.washingtonpost.com/opinions/bernie-sanderss-fiction-filled-campaign/2016/01/27/cd1b2866-c478-11e5-9693-933a4d31bcc8_story.html?postshare=9101453970877610&tid=ss_tw
http://www.huffingtonpost.com/entry/sanders-health-plan-cost_us_56a8ff99e4b0f6b7d5447ee8?section=politics
In practice, Thorpe says, doing so in the U.S. would require dramatic changes that neither the health care industry nor the public would tolerate, at least in one fell swoop. And that, Thorpe told HuffPost, makes the Sanders plan “completely implausible” without major changes.

My Good Babushka
(2,710 posts)is the assumption that any new system would have to absorb, dollar for dollar, the over-inflated prices in health care caused by the collusion of the hospitals, pharmaceutical and insurance industries, and I don't think that's the case.
Recursion
(56,582 posts)That's what I'm saying: doctors and hospitals need to make about half of what they do now, while serving 80 million more people.
My Good Babushka
(2,710 posts)the battle of the monopolies. Here in Western Pennsylvania we have UPMC and Highmark constantly at odds, screwing up everyone's access, spending untold fortunes battling each other for supremacy, and I don't even know what column they would put those PR, whole page ads, TV spots, and lobbying costs under. I would gladly end health care empires to get everyone covered.

JonathanRackham
(1,604 posts)How much of the listed salaries go to pay for malpractice insurance? Would limits on malpractice awards rein in salaries?
Recursion
(56,582 posts)So, it's not really even a rounding error on this. However, there are also increased costs from defensive medicine; those are notoriously hard to quantify, but real. Kaiser says about $40 billion, but even they admit that's just a somewhat educated guess.
JonathanRackham
(1,604 posts)Of course different doctors pay different rates depending upon risk. I hear about US medical malpractice lawsuits in the news but never on the BBC or from Canada. I wonder how the rest of the world fairs?
Recursion
(56,582 posts)The rest of the world also doesn't sue a fast food restaurant when their coffee burns them*. We're just a litigious society.
* Yes, yes, I know, she only sued for the amount of her hospital bills and the jury upped the award because the manager was such a dickbag on the stand. It's just an example people know.
JonathanRackham
(1,604 posts)Recursion
(56,582 posts)It would knock down about $50 billion of that spending, or roughly what we spend on R&D annually. That could double our research efforts right there, or those savings could go to other places. But it's just one reason among dozens that our health care is so expensive, and they're all kind of knotted together, and financing simply isn't Alexander's sword*.
* https://en.wikipedia.org/wiki/Gordian_Knot if anyone is unfamiliar.
JonathanRackham
(1,604 posts)Just think there should be caps on lawsuits. Some lawyers are better fishermen than others. Insurance executives and malpractice lawyers have better houses and cars than doctors. Doctors bring more value to life, excess insurance and Lawyers steal their value.
DanTex
(20,709 posts)As you've pointed out, tort reform is a red herring when it comes to healthcare. But in the larger context, it's a right-wing push to make it harder to sue corporations for damages.
Recursion
(56,582 posts)That said I think there has to be a better way to deal with it than some of the defensive medicine "best practices" (cough cough) that have evolved, and, yeah: that way might involve damages caps in some form.
taught_me_patience
(5,477 posts)My wife pays $15,000/yr in malpractice insurance. That amounts to a cost of 2% of gross and less than 10% on net profit.
Human101948
(3,457 posts)Whenever I ask anyone “how much do you think I pay for my malpractice insurance?” their answer never fails to amuse me. People often guess that I pay anywhere from $30,000 to $150,000 per year (as if I could afford that). When I tell them what I actually pay, they’re usually shocked and some people have even gone so far as to tell me I must be wrong. I write the check each quarter so I know how much it is. Well, seeing is believing, so here is my malpractice bill for all of 2015.
That’s right, $4,926.63 for the whole year! (It says $5025.63 because they want a voluntary $99.00 yearly PAC contribution that they add to the the bill.) This is the fifth straight year that I’ve paid less than $5,000 for my malpractice and my premiums have been as low as $3,000 for the year.


http://www.forbes.com/sites/rickungar/2010/09/07/the-true-cost-of-medical-malpractice-it-may-surprise-you/#47aceb429ccd
redwitch
(14,941 posts)Their business should be providing the best health care to the most people. Why do they have to make a profit?
Doctors should make a good living. They also shouldn't have to spend a brazillion dollars to become doctors.
Recursion
(56,582 posts)That's why I think O'Malley's plan is much, much better. Under his plan, hospitals will have to (or at least be "strongly encouraged to" adopt global budgeting based on the population they serve. If you serve 100,000 people, your budget is $50 million (I'm absolutely making these numbers up, as a warning). If those people live in high poverty with high lead contamination in the water, it's $70 million. If they are affluent suburbanites, it's $45 million.
adopt global budgeting based on the population they serve. If you serve 100,000 people, your budget is $50 million (I'm absolutely making these numbers up, as a warning). If those people live in high poverty with high lead contamination in the water, it's $70 million. If they are affluent suburbanites, it's $45 million.
The Federal government will provide an operating grant equal to some percentage (I think 10% under O'Malley's plan; I'd like it to be much higher but obviously it's the art of the possible, and all) and HHS number-crunchers will tell you what you can charge Medicare for all of your services to make that happen.
Also, under his plan (this is a bigger stretch, realistically, but an awesome idea), if you take Medicare, you have to publish those costs, and offer those same costs to people paying cash.
redwitch
(14,941 posts)But if we put all of it on the table and work on it we could have the best health care anywhere in the world AND make sure we all have access to it no matter where we live. We have to want it and work for it. Good for Martin and Bernie for addressing it so vigorously and thoughtfully. We can't go on as we are.

Nanjeanne
(4,915 posts)also studies show that caps in states have not reduced healthcare costs. And I for one do not wish to see patients that have been damaged by poor care have limited ability to sue. Frivolous cases don't get far in the courts. And there already are many states with caps. Plus medical malpractice is not ridiculously expensive. For most it is between $4-7,000. Obviously for surgeons it is more. Easily more money is spent in salaries for billing that will disappear.
billing and back office support costs significantly more in offices and hospitals than with single payer. Again savings for doctors and hospitals when enacted.
Recursion
(56,582 posts)or "all-payer", as campaign operatives insist on calling it.
That is what Maryland adopted under governor O'Malley, and Maryland is the only state to have seen hospital costs go down in the past decade.

tazkcmo
(7,300 posts)
DemocratSinceBirth
(99,708 posts)lumberjack_jeff
(33,224 posts)DemocratSinceBirth
(99,708 posts)The person providing the service gets to determine how much he he or she will charge for it and the person receiving the service gets to determine how much he or she will pay for it. Nothing in the previous sentence suggests I oppose caps on fees for any service when they become so high they circumvent the public good.
That being said, the thirteenth Amendment provides limits on commandeering the labor of others.
lumberjack_jeff
(33,224 posts)But patients have no choice about getting the repair.
The AMA controls the supply of doctors by creating arbitrary barriers to entry in the trade, including limiting the number of med schools.
The AMA is just another lobbying group whose influence should be purged from DC.
DemocratSinceBirth
(99,708 posts)Physicians make huge sacrifices, which I can elaborate on if you want but they should be self evident, and it is going to require incentives well behind what is customary for most other professions to incentivize a person to become one.
lumberjack_jeff
(33,224 posts)Internship? Residency? All arbitrary bullshit to flush qualified doctors out of the workforce to keep prices high.
Most of what you describe as sacrifices are actually tactics established by the AMA to keep labor scarce.
polly7
(20,582 posts)have been advocating for a single payer system for years.
DU'er Uncle Joe started a thread:
http://www.democraticunderground.com/12511080467
Doctors group welcomes national debate on ‘Medicare for All’
FOR IMMEDIATE RELEASE, January 22, 2016
Physicians for a National Health Program, a nonprofit, nonpartisan organization of 20,000 doctors who support single-payer national health insurance, released the following statement today by its president, Dr. Robert Zarr, a Washington, D.C., pediatrician.
The national debate on single-payer health reform, or "Medicare for All," that has emerged in the course of the presidential primaries is a welcome development. But unfortunately a number of misrepresentations about single-payer national health insurance – and the prospects for its attainment – have crept into the dialogue and are potentially misleading the public.
Most of these misrepresentations, or myths, have been decisively refuted by peer-reviewed research. They include the following:
Myth: A single-payer system would impose an unacceptable financial burden on U.S. households. Reality: Single payer is the only health reform that pays for itself. By replacing hundreds of insurers and thousands of different private health plans, each with their own marketing, enrollment, billing, utilization review, actuary and other departments, with a single, streamlined, tax-financed nonprofit program, more than $400 billion in health spending would be freed up to guarantee coverage to all of the 30 million people who are currently uninsured and to upgrade the coverage of everyone else, including the tens of millions who are underinsured. Co-pays and deductibles, which have been rapidly rising under the Affordable Care Act, would be eliminated. Further, the single-payer system’s bargaining clout would rein in rising costs for drugs and medical supplies. Lump-sum budgets for hospitals and capital planning would control costs even more.
A recent study shows 95 percent of U.S. households would come out financially ahead under an improved version of Medicare for all. The graduated, progressively structured tax burden would be based on ability to pay, and the heavy cost to average U.S. households of private insurance premiums, co-pays, deductibles, and many currently uncovered services would be eliminated. Patients could go to the doctor or hospital of their choice, and would no longer be restricted to proprietary networks. Multiple studies over a period of several decades, including by the General Accountability Office and the Congressional Budget Office, show that a single-payer system would provide universal coverage at a much lower cost, per capita, than we are spending now. International experience confirms it. Even our traditional Medicare program, which falls short of a true single-payer system, has much lower overhead than private insurance, and shows that publicly financed programs can deliver affordable, reliable care.
A single-payer system would also greatly diminish the administrative burden on our nation’s physicians and hospitals, freeing up physicians, in particular, to concentrate on doing what they know best: caring for patients.
(snip)
http://www.pnhp.org/news/2016/january/doctors-group-welcomes-national-debate-on-%E2%80%98medicare-for-all%E2%80%99
DemocratSinceBirth
(99,708 posts)My point...
My cousin is a doctor. My fiancee's uncle and aunt are doctors. My best friend's dad was a doctor. My dad put up street signs for a living. I was able to take more vacations than my friend because his dad was so wed to his practice.
My only point is it is going to take incentives, greater than what is customary, to get folks to become doctors.
polly7
(20,582 posts)desirable for medical doctors seem to have no problem. As I stated upthread, many stay for decades and love the communities and people the get to know so well. I know plenty personally - their incentive is providing great health-care, helping people who need it - the reason they became doctors in the first place.
Just as the nurses, paramedics, lab-techs, etc. who could be working in cities and not having to put in extra hours at times, being able to take advantage of the variety of services that cities offer - we all stay because we prefer to.
DemocratSinceBirth
(99,708 posts)My only point is it is a tough job and those that do it deserves to be well compensated. I would also include nurses in that equation.
polly7
(20,582 posts)well compensated. We're a team.
DemocratSinceBirth
(99,708 posts)Nurses pull twelve hour shifts. Doctors are awoke at 2 in the morning to pin the hip of someone who has fell. Residents goe a day without sleeping. You have to pay attention from high school up. You are exposed to illness...
Tough job.
If I were smart enough to be a doctor I think I would be a chemist.
polly7
(20,582 posts)If I hadn't made such stupid decisions when I was younger, I would have tried to make it happen. My niece is a physician in Sylvan Lake Alberta - so young, but she worked very, very hard to get her license and absolutely loves it, she hopes to go on to specialize in Obstetrics.
DemocratSinceBirth
(99,708 posts)I sucked at chemistry.
polly7
(20,582 posts)DemocratSinceBirth
(99,708 posts)When I was a kid I loved Social Studies and Current Events; Math and Biology, not so much.
I also should have paid more attention in English. I'm not sure if I just used the semicolon right.
It reflects two outlooks in life. Folks can decide which is better...You can pick a few things you do well at and try to get even better or you can pick things you do poorly and try to do them well.
Maybe I picked the path of least resistance...Too late now...
polly7
(20,582 posts)sometimes end up working 48 hour shifts. My co-worker and I didn't sleep for three days one horrible winter week - we were short an EMT - then, we worked in the nursing home during the day (we all had to get Special Care Aide training and certificates - this is only in a few districts that don't have the quantity of calls to justify paying EMT'S/Paramedics to sit around waiting) and left if called out and were on call during the night. We had two serious MVA's and multiple transfers from the nursing home and hospital. It was unreal, but that doesn't happen often. My point is - our system wouldn't work without everyone in the team sacrificing in some way - at times - to keep it going. But that's what we all expected when we decided to train for it and choose a place to work. Doctors here, at least in rural areas - I don't know about those in the cities as I only trained and stayed in several in Alberta for a few years at a time - are the biggest part of the team, and they choose to be. It if was unbearable or something they couldn't deal with - they'd leave.
Sienna86
(2,148 posts)It will promote medical staff who purely wish to help,others, not a career with with a big salary. It will cull those few medical corporatists who make most of the money.
Final_Sign
(1 post)I've been lurking for a while but this thread made me register. Lots of good discussion in this thread.
I'm a physician, a radiologist to be specific. I think most physicians would be in favor of a "single payer" type system when you look at the simplicity factor. Dealing with insurance is very time consuming. You have to pre-certify patients for procedures/studies, constantly play the game of documentation so you can get reimbursed for your time, pay people to figure out the correct way to code everything and submit info to insurance companies, then fight insurance companies after they deny you payment for various reasons. All of that takes lots of time and resources and adds to the total cost of healthcare.
A "single payer" system would help to reduce some of that, but it would not eliminate it. Physicians still have to jump through hoops when dealing with Medicare, Medicaid, or when working in the VA system. Most physicians imagine any government run single payer system would be similar to the current government run systems we already deal with and they are not "simple" by any means. We'd still be fighting with the government to get paid for the work we do.
What does make physicians nervous about "single payer" is when you start discussing cost control. As mentioned in the OP, the Sanders plan calls for tons of cost reduction but doesn't really explain where that comes from. Eliminating overhead will help some, but it will only put a tiny dent in the overall cost of healthcare.
So how do we control costs? Most doctors will openly admit there is a huge amount of waste in healthcare. We order too many studies, we admit patients that don't need to be admitted, we send patients to a specialist that probably don't need it, etc. Why does all that happen? Are we trying to milk the system and get paid as much as we can? NO, doctors contribute to tons of waste out of FEAR. We do tons of stuff that doesn't need to be done because we are playing the CYA game (cover your ass). We pay tons of money for malpractice insurance but still get sued frequently even when doing nothing wrong. Doctors are no longer allowed to just use their "clinical judgement" based on our extensive education and work experience. We now are forced to prove everything beyond any reasonable doubt so that in the slim chance something does go wrong we don't get sued like crazy. I understand the need to protect patients and give them a way to fight against true malpractice, but I think we've swung the pendulum too far in that direction and we have created a hostile environment for physicians that makes us treat patients in a way that adds unneeded cost.
I interact with physicians who have worked in other countries before and in those other locations that have significantly reduced healthcare costs, there is a huge difference. Doctors in those other places are allowed to use their clinical judgement. They can see a patient in the ER and say, "I think you'll be ok, no imaging or surgery needed, just go home and if it gets worse come back to the ER". But in the USA, that patient is going to get a full range of blood work, CT scan, and a surgical consult even if the ER doc doesn't think they need it. We do it all just so that patient doesn't go home and end up suing the ER doc because they missed something subtle.
Tort reform would help to protect doctors in the US, but it will take years to make doctors change their practice habits and reduce cost by eliminating the waste from "CYA medicine".
We also have a huge problem with end of life care in the USA. We spend a ton of money keeping people alive a little bit longer before they die. We are afraid of death and dying and many end of life treatment decisions are not discussed until the bitter end and then emotions run high and everybody wants to do everything they possibly can to keep grandpa alive. We could reduce tons of cost by having logical discussions about stopping some of that spending, but that's where you get into the "death panels" that strikes fear into everyone's hearts. We can reduce tons of healthcare cost if we just stop offering some things to some patients such as not performing certain surgeries on patients over a certain age (common in other countries) or doing fewer resuscitations on elderly patients or patients who are already terminal. I see many old patients with terminal illness who are still requesting they be a full code. IMHO, we should utilize more services like HOSPICE where we allow patients with terminal illnesses to be kept comfortable, but we don't blow tons of money bringing them back to life everytime there heart stops. But you bring this topic up with some people and all they year is "omg they want to kill grandpa!!!"
So, do you have to cut all doctors salaries by 50% to cut costs? No, there are many ways to cut costs, but I'm not sure our society is ready to make the necessary commitments. Doctors fear a single payer would end up with the government cutting costs by basically telling us how to do our jobs.
CaliforniaPeggy
(149,525 posts)And thank you for you very clear description of the problems we face.
I hope you will enjoy being here. There are many lively conversations going on, and you've just made a considerable contribution to them.
Welcome!
Recursion
(56,582 posts)And I find that lack of specificity alarming. O'Malley, at least, is very clear about how global rate-setting will affect providers; Sanders, not so much.
lumberjack_jeff
(33,224 posts)Surely if the national security interests of the US demand bringing in hundreds of thousands of foreign programmers, the same logic holds true for doctors.
I only care that doctors are paid well enough to assure that med schools remain filled.
99Forever
(14,524 posts) Recursion
(56,582 posts)This is pretty basic arithmetic. Which rows do you want to be lower, and by how much?
99Forever
(14,524 posts)Start there.
Recursion
(56,582 posts)Seriously. Where does the other trillion dollars come from?
taught_me_patience
(5,477 posts)Would anybody on this board like a 40% pay cut? I would fight this tooth and nail.
Travis_0004
(5,417 posts)
Bjornsdotter
(6,123 posts)...he lives quite well and has no issue on the money he makes. He was offered a position in the states....he turned it down.
Apparently money isn't everything.
taught_me_patience
(5,477 posts)Whether you agree with Bernie Sander's plan or not (I don't), this is the only way to have the cost savings that he's touting. Bernie will not say it because it will obviously cause a shortage in doctors in this country. I cannot recommend this post enough... thank you.
nolabels
(13,133 posts)The administrative and other overhead devices is what is screwing up health care. With single payer things can be more correctly focused on health care rather than the next money gimmick. A detailed unfettered plan on what is to worked on is always the most effective way to get things done
Recursion
(56,582 posts)No. I listed the costs in the OP. Overhead, public and private, including profit for insurers, is about $240 Billion of the $3 Trillion we spend every year.
Most of our spending is going to hospitals and doctors. If we expect Single Payer to save us money, hospitals and doctors have to make less money.
LittleBlue
(10,362 posts)Their salaries are a huge reason why our healthcare costs are spiraling out of control. Doctors with private practices making $500k per year is too high for everyone to have access.

Hiraeth
(4,805 posts)and Dietary are DUE RAISES .... especially HOUSEKEEPING and DIETARY .... $15.00 minimum wage ..... start there and then go up the ladder and adjust accordingly. I would expect to see some need no adjustment either direction while admin and mgment may actually need to take a CUT in PAY.
Hiraeth
(4,805 posts)NOT burdened with STUDENT LOANS.

Dont call me Shirley
(10,998 posts)safety laws then there won't be as many sick people.
Autumn
(44,982 posts)a crumbling infrastructure. In other words yes, I am fine if doctors and hospitals make half of what they make now.
Jenny_92808
(1,342 posts)at much lower costs to the populous. Unless you think that the richest of the richest should be able to steal from all the people of the USA resulting in countless unnecessary deaths?
Jenny_92808
(1,342 posts)so the richest of the richest can make more money?
Recursion
(56,582 posts)Do you?